
The Muscular System Anatomy
Muscles of the Head, Neck & Back
Objectives
- Locate the muscles of the head, neck & back on laboratory charts and models.
- Recognize on the models the origin, insertion, and action of the muscles of the head, neck & back.
- Describe and demonstrate the action of the muscles of the head, neck & back.
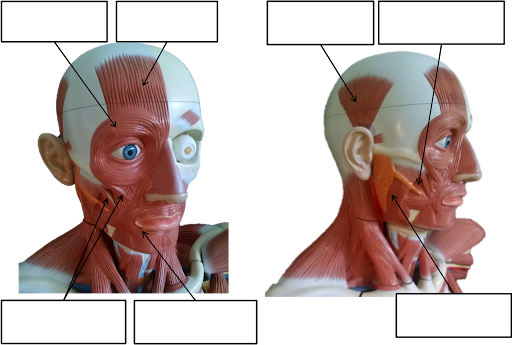
Muscles of Facial Expression
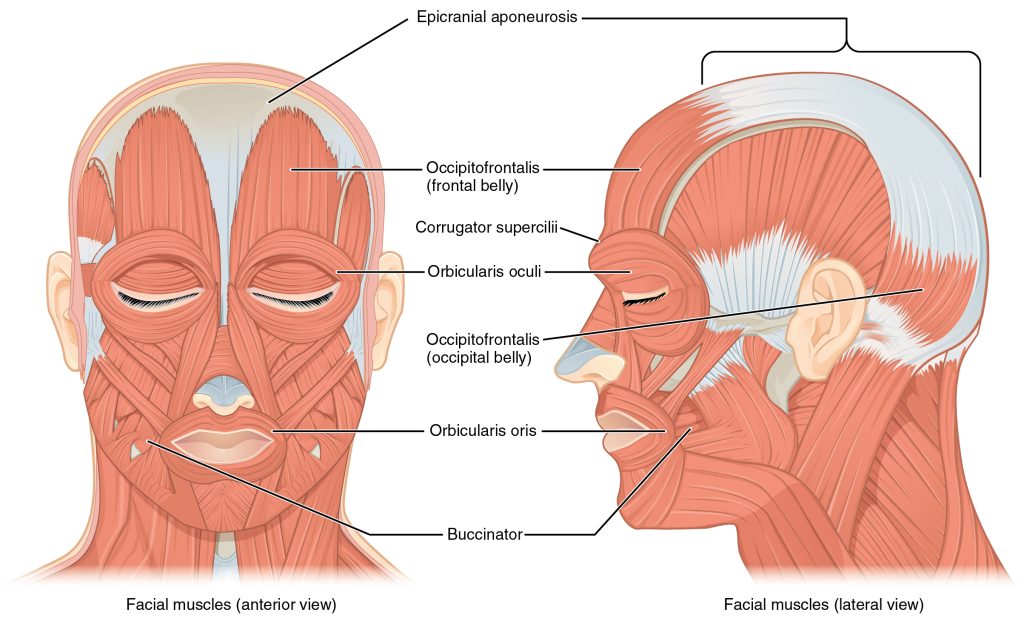
The muscles of facial expression originate from the surface of the skull or the fascia (connective tissue) of the face. The insertions of these muscles have fibers intertwined with connective tissue and the dermis of the skin. Because the muscles insert in the skin rather than on bone, when they contract, the skin moves to create facial expressions.
Brow
| Muscle | Origin | Insertion | Action | Innervation |
| Occipitofrontalis, frontal belly | Epicraneal aponeurosis | Underneath skin of forehead | Furrowing brow | Facial nerve |
| Occipitofrontalis, occipital belly | Occipital bone; mastoid process (temporal bone) | Epicraneal aponeurosis | Unfurrowing brow | Facial nerve |
| Corrugator supercilii | Frontal bone | Skin underneath eyebrow | Draws eyebrows medially and downward; frowning | Facial nerve |
Nose
| Muscle | Origin | Insertion | Action | Innervation |
| Nasalis | Maxilla | Nasal bone | Widens nostrils | Facial nerve |
Mouth
| Muscle | Origin | Insertion | Action | Innervation |
| Levator labii superioris | Maxilla | Underneath skin at corners of the mouth; orbicularis oris | Elevates upper lip | Facial nerve |
| Depressor labii inferioris | Mandible | Underneath skin of lower lip | Draws lower lip downward | Facial nerve |
| Depressor angulus oris | Mandible | Underneath skin at corners of the mouth | Opening mouth and sliding lower jaw left and right | Facial nerve |
| Zygomaticus major | Zygomatic bone | Underneath skin at corners of the mouth (dimple area); orbicularis oris | Draws angle of mouth upward and laterally; smiling | Facial nerve |
| Orbicularis oris | Tissue surrounding lips | Underneath skin at corners of the mouth | Shaping of lips (as during speech) | Facial nerve |
| Buccinator | Maxilla, mandible; sphenoid bone (via pterygomandibular raphae) | Orbicularis oris | Lateral movement of cheeks (e.g., sucking on a straw; also used to compress air in mouth while blowing) | Facial nerve |
| Risorius | Fascia of parotid salivary gland | Underneath skin at corners of the mouth | Draws angle of mouth laterally. | Facial nerve |
| Mentalis | Mandible | Underneath skin of chin | Elevates and protrudes lower lip ands skin of the chin | Facial nerve |
Muscles of the Eye
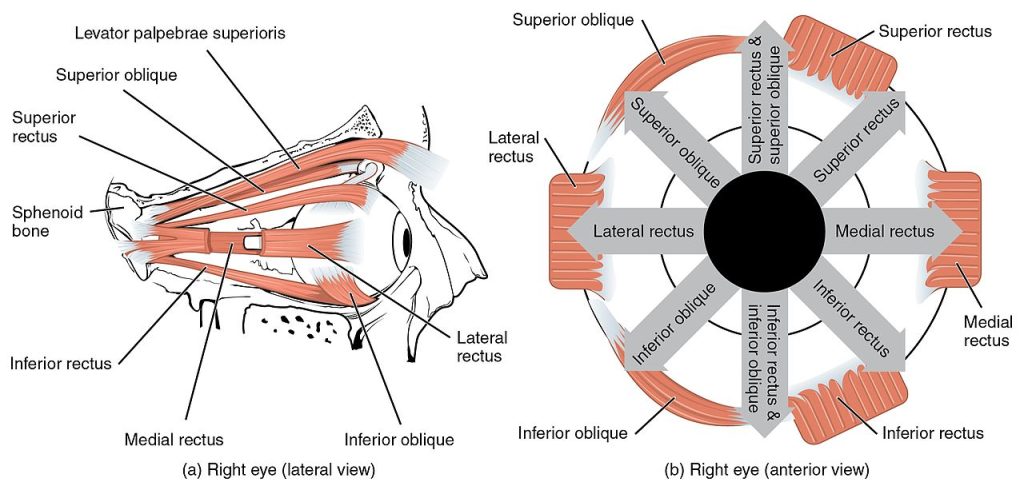
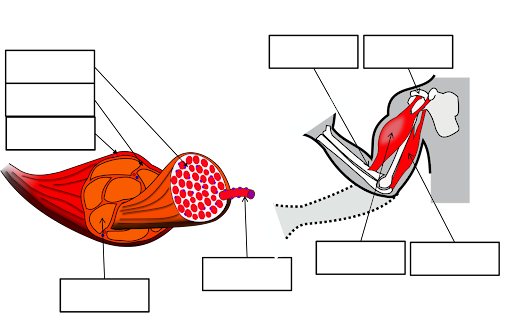
The movement of the eyeball is under the control of the extra ocular (extrinsic) eye muscles, which originate from the bones of the orbit and insert onto the outer surface of the white of the eye. These muscles are located inside the eye socket and cannot be seen on any part of the visible eyeball. If you have ever been to a doctor who held up a finger and asked you to follow it up, down, and to both sides, he or she is checking to make sure your eye muscles are acting in a coordinated pattern.
Muscles of the Eyes
(a) The extraocular eye muscles originate outside of the eye on the skull. (b) Each muscle inserts onto the eyeball.
| Muscle | Origin | Insertion | Action/Movement | Innervation |
| Inferior rectus | Sphenoid around optic canal (Annulus of Zinn) | Inferior, medial surface of the eyeball | Eye looks down, depression. | Oculomotor nerve (N II) |
| Medial rectus | Sphenoid around optic canal (Annulus of Zinn) | Medial surface of eyeball | Eye looks medially, adduction | Oculomotor nerve (N II) |
| Superior rectus | Sphenoid around optic canal (Annulus of Zinn) | Superior, anterior surface of eyeball | Eye looks up, elevation | Oculomotor nerve (N II) |
| Lateral rectus | Sphenoid around optic canal (Annulus of Zinn) | Lateral, anterior surface of eyeball | Eye looks laterally, abduction | Abducens nerve (N VI) |
| Inferior oblique | Maxilla, anterior area of orbit | Inferior, lateral surface of eyeball | Eye rolls, looks up and laterally, excyclotorsion | Oculomotor nerve (N III) |
| Superior oblique | Sphenoid at optic canal | Superior, lateral surface of eyeball | Eye rolls, looks down and laterally, incyclotorsion | Trochlear nerve (N VI) |
| Levator palpebrae superioris | Sphenoid | Tarsal plate of upper eyelid | Elevates, retracts upper eyelid | Oculomotor nerve (N III) |
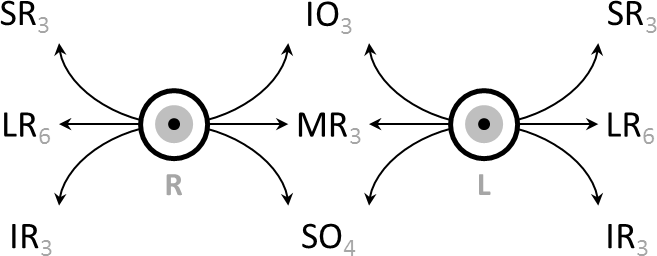
Movement Coordination
Intermediate directions are controlled by simultaneous actions of multiple muscles. When one shifts the gaze horizontally, one eye will move laterally (toward the side) and the other will move medially (toward the midline). This may be neurally coordinated by the central nervous system, to make the eyes move together and almost involuntarily. This is a key factor in the study of strabismus, namely, the inability of the eyes to be directed to one point.
There are two main kinds of movement: conjugate movement (the eyes move in the same direction) and disjunctive (opposite directions). The former is typical when shifting gaze right or left, the latter is convergence of the two eyes on a near object. Disjunction can be performed voluntarily, but is usually triggered by the nearness of the target object. A “see-saw” movement, namely, one eye looking up and the other down, is possible, but not voluntarily; this effect is brought on by putting a prism in front of one eye, so the relevant image is apparently displaced. To avoid double vision from non-corresponding points, the eye with the prism must move up or down, following the image passing through the prism. Likewise conjugate torsion (rolling) on the anteroposterior axis (from the front to the back) can occur naturally, such as when one tips one’s head to one shoulder; the torsion, in the opposite direction, keeps the image vertical.
The muscles show little inertia – a shutdown of one muscle is not due to checking of the antagonist, so the motion is not ballistic.
Eye Examination
The initial clinical examination of the extra-occular eye muscles is done by examining the movement of the globe of the eye through the six cardinal eye movements. When the eye is turned out (temporally) and horizontally, the function of the lateral rectus muscle is tested. When the eye is turned in (nasally) and horizontally, the function of the medial rectus muscle is being tested. When turning the eye down and in, the inferior rectus is contracting. When turning it up and in the superior rectus is contracting. Paradoxically, turning the eye up and out uses the inferior oblique muscle, and turning it down and out uses the superior oblique. All of these six movements can be tested by drawing a large “H” in the air with a finger or other object in front of a patient’s face and having them follow the tip of the finger or object with their eyes without moving their head. Having them focus on the object as it is moved in toward their face in the midline will test convergence, or the eyes’ ability to turn inward simultaneously to focus on a near object.
To evaluate for weakness or imbalance of the muscles, a penlight is shone directly on the corneas. Expected normal results of the corneal light reflex is when the penlight’s reflection is located in the center of both corneas, equally.
In The Lab
- Review the muscles of the eye in the images and tables provided
- Examine the eye model and eye muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each eye muscle using your eyes and your lab partners.
Muscles That Move the Lower Jaw/ Mastication
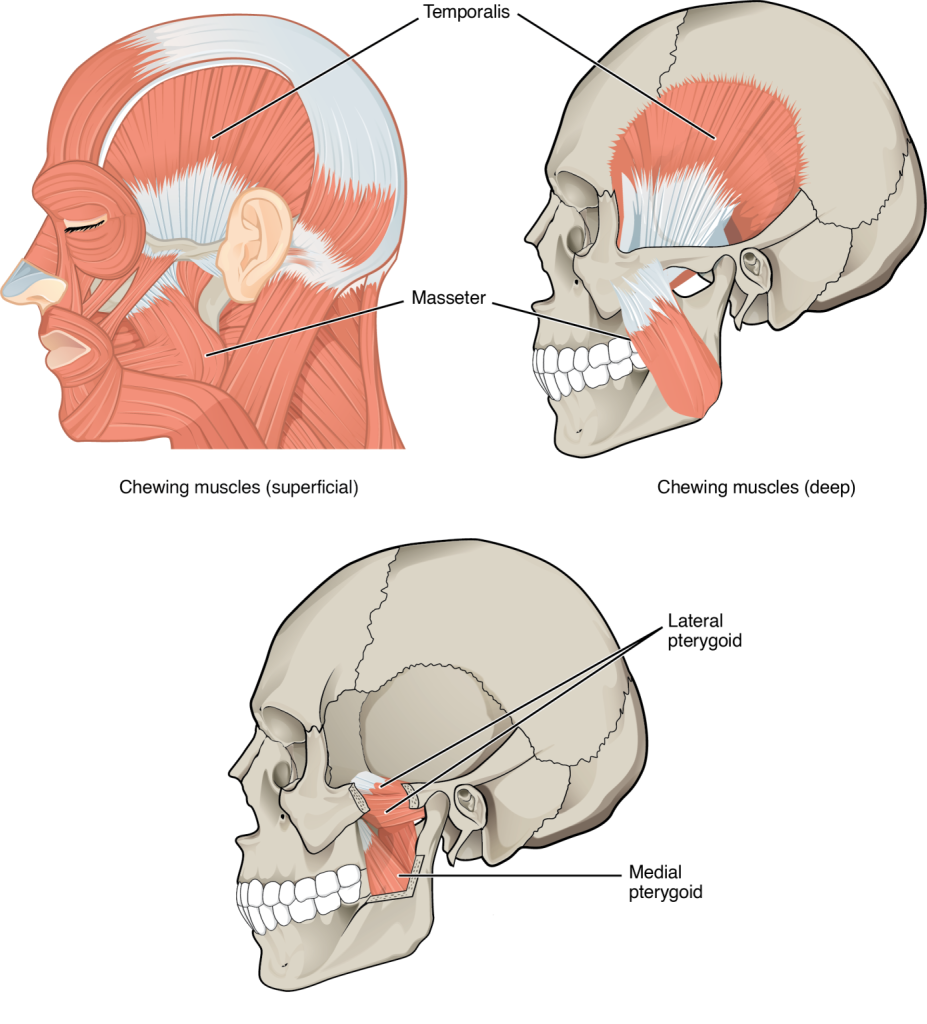
In anatomical terminology, chewing is called mastication. Muscles involved in chewing must be able to exert enough pressure to bite through and then chew food before it is swallowed. The masseter muscle is the prime mover muscle for chewing because it elevates the mandible (lower jaw) to close the mouth, and it is assisted by the temporalis muscle, which retracts the mandible. You can feel the temporalis move by putting your fingers to your temple as you chew. The medial pterygoid and lateral pterygoid muscles provide assistance in chewing and moving food within the mouth by moving the mandible laterally and medially to grind food between the molars.
Muscles That Move the Lower Jaw
The muscles that move the lower jaw are typically located within the cheek and originate from processes in the skull. This provides the jaw muscles with the large amount of leverage needed for chewing.
| Muscle | Origin | Insertion | Action | Innervation |
| Masseter | Zygomatic arch | Lateral surface of mandibular arch | Elevates mandible and closes jaw, aids chewing | Mandibular branch of Trigeminal nerve (N V) |
| Temporalis | Temporal lines of skull | Coronoid process of mandible | Elevates mandible, pulls lower jaw in under upper jaw | Mandibular branch of Trigeminal nerve (N V) |
| Medial pterygoid | Lateral pterygoid plate | Medial area of mandibular ramus | Elevates the mandible & closes jaw, pushes lower jaw out under upper jaw; moves lower jaw side-to-side | Mandibular branch of Trigeminal nerve (N V) |
| Lateral pterygoid | Lateral pterygoid plate | Medial area of mandibular ramus | Protrudes the mandible, opens jaw, pushes lower jaw out under upper jaw; moves lower jaw side-to-side | Mandibular branch of Trigeminal nerve (N V) |
In The Lab
- Review the muscles of mastication in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle using yours and your lab partners.
Muscles of the Tongue
Although the tongue is obviously important for tasting food, it is also necessary for mastication, deglutition(swallowing), and speech. Because of its mobility, the tongue facilitates complex speech patterns and sounds.Tongue muscles can be extrinsic or intrinsic. Extrinsic tongue muscles insert into the tongue from outside origins, and the intrinsic tongue muscles insert into the tongue from origins within it. The extrinsic muscles move the whole tongue in different directions, whereas the intrinsic muscles allow the tongue to change its shape (such as, curling the tongue in a loop or flattening it).
The extrinsic muscles all include the word root glossus (glossus = “tongue”), and the muscle names are derived from where the muscle originates. The genioglossus (genio = “chin”) originates on the mandible and allows the tongue to move downward and forward. The styloglossus originates on the styloid process of the temporal bone, and allows upward and backward motion. The palatoglossus originates on the soft palate to elevate the back of the tongue, and the hyoglossus originates on the hyoid bone to move the tongue downward and flatten it.
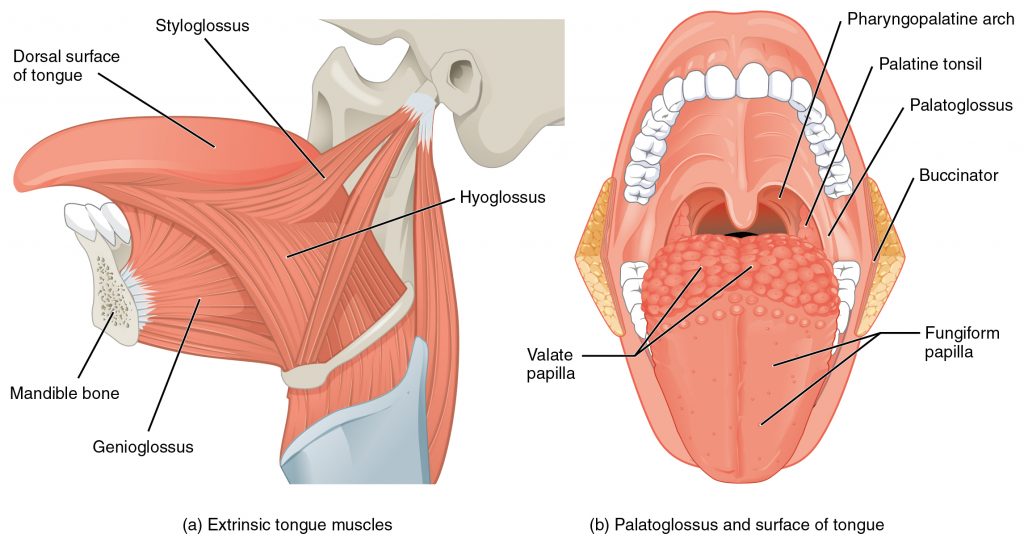
Muscles that Move the Tongue
| Muscle | Origin | Insertion | Action | Innervation |
| Genioglossus | Medial surface of mandible | Hyoid bone, body of tongue | Depresses & protracts tongue | Hypoglossal nerve (N XII) |
| Hyoglossus | Greater horn and body of hyoid bone | Side of tongue | Depresses & retracts tongue | Hypoglossal nerve (N XII) |
| Palatoglossus | Anterior surface of soft palate | Side of tongue | Elevates tongue, depresses soft palate | Internal branch of accessory nerve ( N XI) |
| Styloglossus | Styloid process of temporal bone | Side to tip of tongue base | Retracts tongue, elevates side of tongue | Hypoglossal nerve (N XII) |
Muscle of the Anterior Neck
The muscles of the anterior neck assist in deglutition (swallowing) and speech by controlling the positions of the larynx (voice box), and the hyoid bone, a horseshoe-shaped bone that functions as a foundation on which the tongue can move. The muscles of the neck are categorized according to their position relative to the hyoid bone. Suprahyoid muscles are superior to it, and the infrahyoid muscles are located inferiorly.
The suprahyoid muscles raise the hyoid bone, the floor of the mouth, and the larynx during deglutition. These include the digastric muscle, which has anterior and posterior bellies that work to elevate the hyoid bone and larynx when one swallows; it also depresses the mandible. The stylohyoid muscle moves the hyoid bone posteriorly, elevating the larynx, and the mylohyoid muscle lifts it and helps press the tongue to the top of the mouth. The geniohyoid depresses the mandible in addition to raising and pulling the hyoid bone anteriorly.
The strap-like infrahyoid muscles generally depress the hyoid bone and control the position of the larynx. The omohyoid muscle, which has superior and inferior bellies, depresses the hyoid bone in conjunction with the sternohyoid and thyrohyoid muscles. The thyrohyoid muscle also elevates the larynx’s thyroid cartilage, whereas the sternothyroid depresses it.
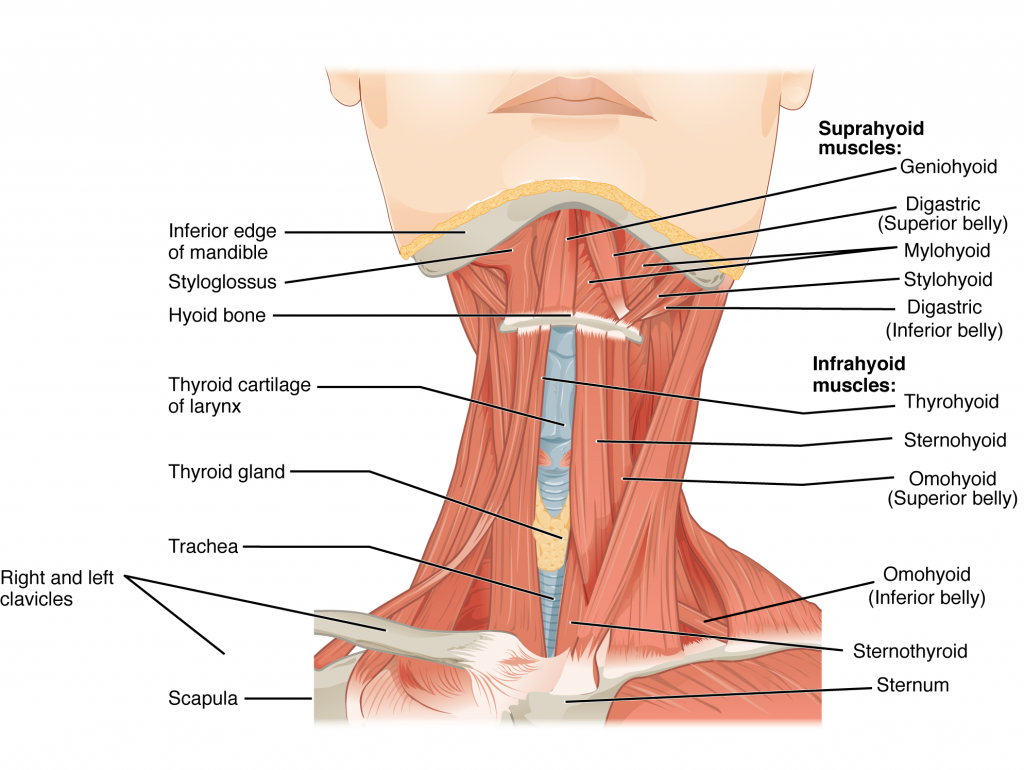 Muscles of the Anterior Neck
Muscles of the Anterior Neck
The anterior muscles of the neck facilitate swallowing and speech. The suprahyoid muscles originate from above the hyoid bone in the chin region. The infrahyoid muscles originate below the hyoid bone in the lower neck.
| Muscle | Origin | Insertion | Action | Innervation |
| Digastric | Mandible at chin and temporal bone | Hyoid bone | Depresses mandible / elevates larynx | Anterior belly: mandibular branch of Trigeminal nerve (N V)
Posterior belly: Facial nerve (N VII) |
| Geniohyoid | Mandible medial surface | Hyoid bone | Depresses mandible / elevates larynx & pulls hyoid bone anteriorly | Spinal nerve C1 via Hypoglossal nerve ( N XII) |
| Mylohyoid | Mandible | Hyoid bone; line of raphe | Elevates hyoid bone & floor of mouth. Depresses mandible | Mandibular branch of Trigeminal nerve (N V) |
| Omohyoid | Superior border of scapula | Hyoid bone | Depresses larynx & hyoid bone | Cervical spine nerves (C2-C3) |
| Sternohyoid | Clavicle & manubrium | Hyoid bone | Depresses larynx & hyoid bone | Cervical spine nerves (C1-C3) |
| Sternothyroid | Dorsal surface of manubrium & first costal cartilage | Thyroid cartilage of larynx | Depresses larynx & hyoid bone | Cervical spine nerves (C1-C3) |
| Stylohyoid | Temporal bone; styloid process | Hyoid bone | Elevates larynx | Facial nerve (N VII) |
| Thyrohyoid | Larynx; thyroid cartilage | Hyoid bone | Elevates thyroid, depresses hyoid bone | Spinal nerve C1- C2, via Hypoglossal nerve ( N XII) |
| Sternocleidomastoid | Clavicular head; to sternal end of clavicle
Sternal head; to manubrium |
Mastoid area of skull & superior nuchal line | Rotates and tilts head to the side, tilts head forward | Accessory nerve ( N XII) & cervical spinal nerves C2-C3) |
Muscles of the Posterior Neck and Back
The posterior muscles of the neck are primarily concerned with head movements, like extension. The back muscles stabilize and move the vertebral column, and are grouped according to the lengths and direction of the fascicles.
The splenius muscles originate at the midline and run laterally and superiorly to their insertions. From the sides and the back of the neck, the splenius capitis inserts onto the head region, and the splenius cervicis extends onto the cervical region. These muscles can extend the head, laterally flex it, and rotate it
The erector spinae group forms the majority of the muscle mass of the back and it is the primary extensor of the vertebral column. It controls extension, lateral flexion, and rotation of the vertebral column, and maintains the lumbar curve. The erector spinae comprises the iliocostalis (laterally placed) group, the longissimus (intermediately placed) group, and the spinalis (medially placed) group.
The iliocostalis group includes the iliocostalis cervicis, associated with the cervical region; the iliocostalis thoracis, associated with the thoracic region; and the iliocostalis lumborum, associated with the lumbar region. The three muscles of the longissimus group are the longissimus capitis, associated with the head region; the longissimus cervicis, associated with the cervical region; and the longissimus thoracis, associated with the thoracic region. The third group, the spinalis group, comprises the spinalis capitis (head region), the spinalis cervicis (cervical region), and the spinalis thoracis (thoracic region).
The transversospinales muscles run from the transverse processes to the spinous processes of the vertebrae. Similar to the erector spinae muscles, the semispinalis muscles in this group are named for the areas of the body with which they are associated. The semispinalis muscles include the semispinalis capitis, the semispinalis cervicis, and the semispinalis thoracis. The multifidus muscle of the lumbar region helps extend and laterally flex the vertebral column.
Important in the stabilization of the vertebral column is the segmental muscle group, which includes the interspinales and intertransversarii muscles. These muscles bring together the spinous and transverse processes of each consecutive vertebra. Finally, the scalene muscles work together to flex, laterally flex, and rotate the head. They also contribute to deep inhalation. The scalene muscles include the anterior scalene muscle (anterior to the middle scalene), the middle scalene muscle (the longest, intermediate between the anterior and posterior scalenes), and the posterior scalene muscle (the smallest, posterior to the middle scalene).
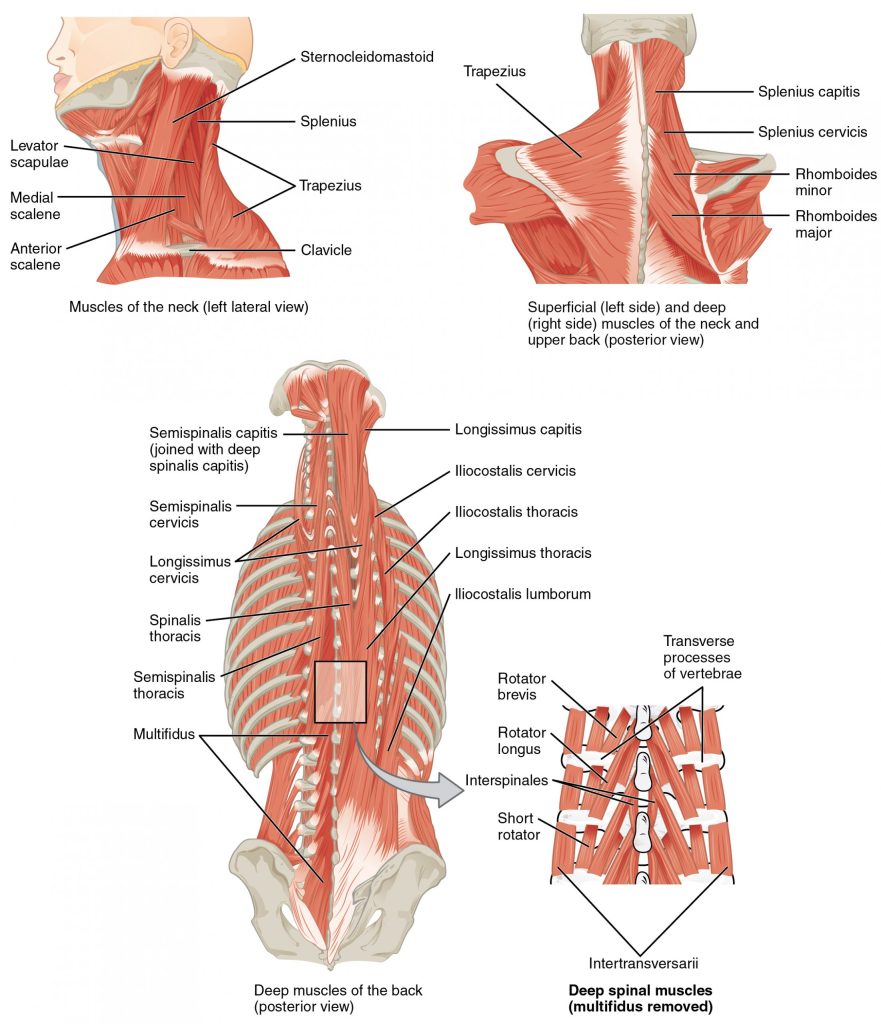
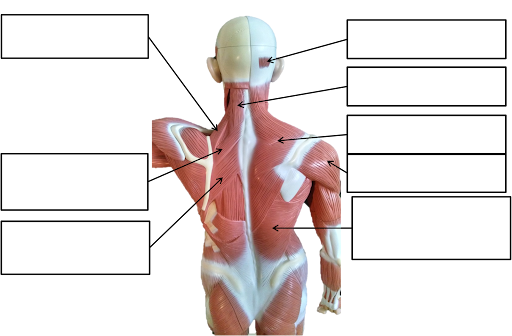
Muscles of the Neck and Back.
The large, complex muscles of the neck and back move the head, shoulders, and vertebral column.
In The Lab
- Review the muscles of the tongue, anterior neck and back in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and practice & describe the action of each muscle.
Review
Muscles are either axial muscles or appendicular. The axial muscles are grouped based on location, function, or both. Some axial muscles cross over to the appendicular skeleton. The muscles of the head and neck are all axial. The muscles in the face create facial expression by inserting into the skin rather than onto bone. Muscles that move the eyeballs are extrinsic, meaning they originate outside of the eye and insert onto it. Tongue muscles are both extrinsic and intrinsic. The genioglossus depresses the tongue and moves it anteriorly; the styloglossus lifts the tongue and retracts it; the palatoglossus elevates the back of the tongue; and the hyoglossus depresses and flattens it. The muscles of the anterior neck facilitate swallowing and speech, stabilize the hyoid bone and position the larynx. The muscles of the neck stabilize and move the head. The sternocleidomastoid divides the neck into anterior and posterior triangles.
The muscles of the back and neck that move the vertebral column are complex, overlapping, and can be divided into five groups. The splenius group includes the splenius capitis and the splenius cervicis. The erector spinae has three subgroups. The iliocostalis group includes the iliocostalis cervicis, the iliocostalis thoracis, and the iliocostalis lumborum. The longissimus group includes the longissimus capitis, the longissimus cervicis, and the longissimus thoracis. The spinalis group includes the spinalis capitis, the spinalis cervicis, and the spinalis thoracis. The transversospinales include the semispinalis capitis, semispinalis cervicis, semispinalis thoracis, multifidus, and rotatores. The segmental muscles include the interspinales and intertransversarii. Finally, the scalenes include the anterior scalene, middle scalene, and posterior scalene.
In The Lab
- Review the muscles of the head using table & figure provided on previous pages.
- Examine and study the head model using the muscle chart provided in lab, locate each muscle (origin, insertion, action & innervation) and describe its action.
- Find the approximate location of the muscles of facial expression on your own face and study & observe their action.
- Explain the difference between axial and appendicular muscles.
- Describe the muscles of the anterior neck.
- Why are the muscles of the face different from typical skeletal muscle?
Muscles of the Abdominal Wall & Thorax
Objectives
- Locate the muscles of the abdominal wall and thorax on laboratory charts and models.
- Recognize on the models the origin, insertion, and action of the muscles of the abdominal wall and thorax.
- Describe and demonstrate the action of the muscles of the abdominal wall and thorax.
It is a complex job to balance the body on two feet and walk upright. The muscles of the vertebral column, thorax, and abdominal wall extend, flex, and stabilize different parts of the body’s trunk. The deep muscles of the body’s core help maintain posture as well as provide stability for movement of the limbs.
Muscles of the Abdomen
There are four pairs of abdominal muscles that make up the abdominal wall: the rectus abdominis, the external abdominal obliques, the internal abdominal obliques and the transverse abdominis.
There are three flat skeletal muscles in the antero-lateral wall of the abdomen. The external oblique, closest to the surface, extend inferiorly and medially, in the direction of sliding one’s four fingers into pants pockets. Perpendicular to it is the intermediate internal oblique, extending superiorly and medially, the direction the thumbs usually go when the other fingers are in the pants pocket. The deep muscle, the transverse abdominis, is arranged transversely around the abdomen, similar to a belt. This arrangement of three bands of muscles in different orientations allows various movements and rotations of the trunk. The three layers of muscle also help to protect the internal abdominal organs in an area where there is no bone.
The linea alba is a white, fibrous band that is made of the bilateral rectus sheaths that join at the anterior midline of the body. These enclose the rectus abdominis muscles that originate at the pubic crest and symphysis, and extend the length of the body’s trunk. Each muscle is segmented by three transverse bands of collagen fibers called the tendinous intersections resulting in the look of “six-pack abs”.
The posterior abdominal wall is formed by the lumbar vertebrae, parts of the ilia of the hip bones, psoas major and iliacus muscles, and quadratus lumborum muscle. This part of the core plays a key role in stabilizing the rest of the body and maintaining posture.
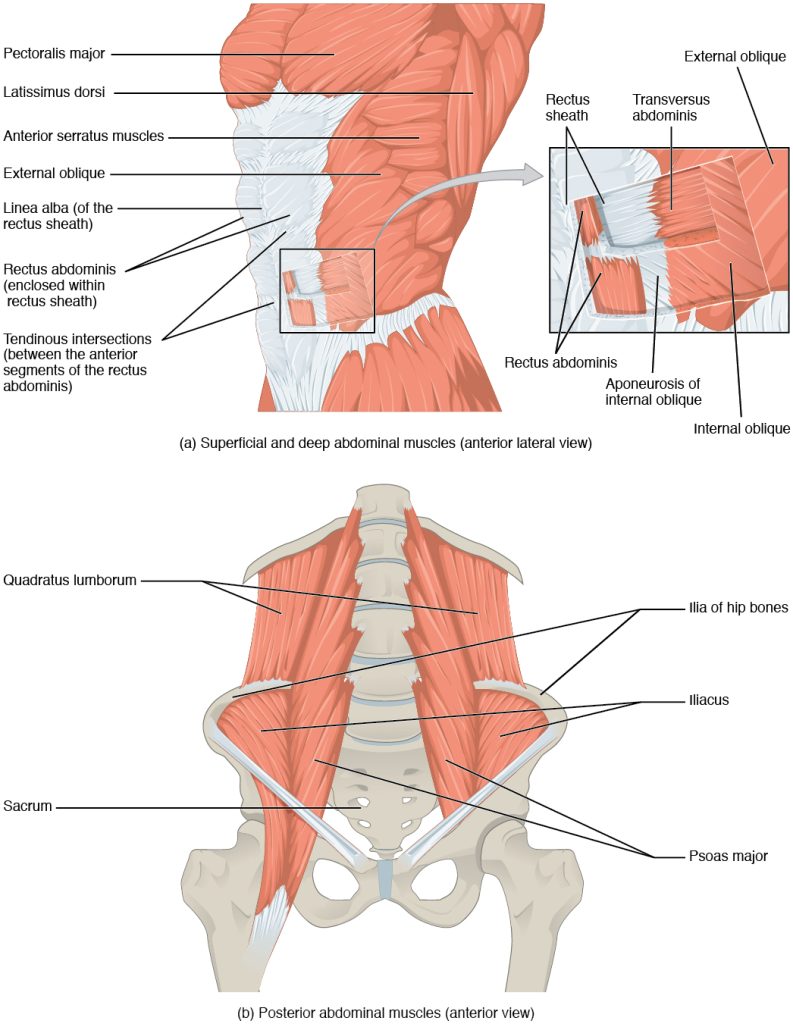
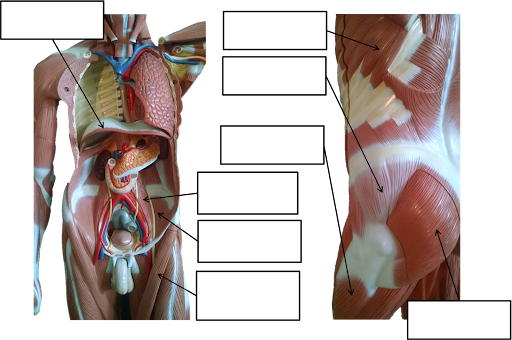
Muscles of the Abdomen
(a) The anterior abdominal muscles include the medially located rectus abdominis, which is covered by a sheet of connective tissue called the rectus sheath. On the flanks of the body, medial to the rectus abdominis, the abdominal wall is composed of three layers. The external oblique muscles form the superficial layer, while the internal oblique muscles form the middle layer, and the transverses abdominus forms the deepest layer.
b) The muscles of the lower back move the lumbar spine but also assist in femur movements.
| Muscle | Origin | Insertion | Action | Innervation |
| External oblique | External & inferior borders of ribs 5-12 | Iliac crest & Linea alba | Bends/flexes spine, compresses abdomen, depresses ribs | Ilioinguinal intercostal, iliohypogastric nerves |
| Internal oblique | Iliac crest, thoracolumbar fascia | Linea alba, xyphoid process, inferior ribs | Bends/flexes spine, compresses abdomen, depresses ribs | Ilioinguinal intercostal, iliohypogastric nerves |
| Transversus abdominis | Ribs 6-12 cartilages, thoracolumbar fascia, iliac crest | Pubis & linea alba | Compresses abdomen | Ilioinguinal intercostal, iliohypogastric nerves |
| Rectus abdominis | Pubis symphysis; superior surface | Ribs 5-7; inferior surfaces of costal cartilages & xiphoid process | Bends/flexes spine, compresses abdomen, depresses ribs | Intercostal nerves (T7-T12) |
| Quadratus lumborum | Iliolumbar ligament & iliac crest | Transverse processes of lumbar vertebrae & last rib | Depress ribs, laterally flexes vertebral column | Thoracic & lumbar spinal nerves |
In The Lab
- Review the muscles of the abdominal wall & thorax in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle with your lab partners.
Muscle of the Thorax
The muscles of the chest serve to facilitate breathing by changing the volume of the thoracic cavity. When you inhale your chest rises increasing the volume of the thoracic cavity. Alternately, when you exhale, your chest falls decreasing the volume of the thoracic cavity.
The Diaphragm
The change in volume of the thoracic cavity during breathing is due to the alternate contraction and relaxation of the diaphragm. It separates the thoracic and abdominal cavities, and is dome-shaped at rest. The superior surface of the diaphragm is convex, creating the elevated floor of the thoracic cavity. The inferior surface is concave, creating the curved roof of the abdominal cavity.
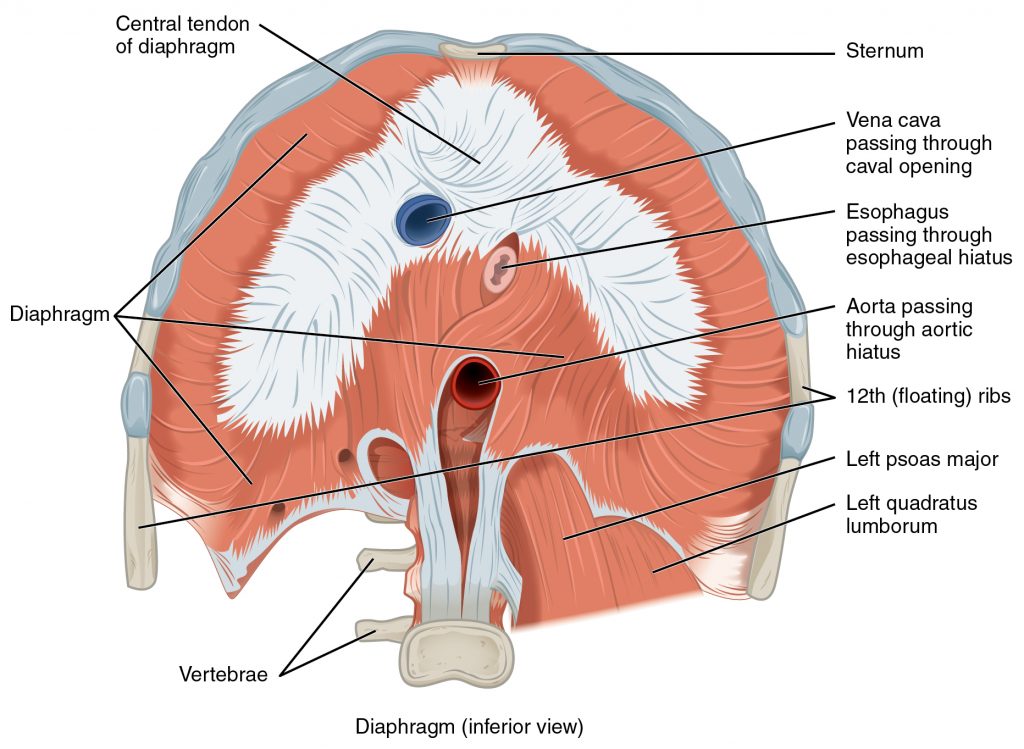
Muscles of the Diaphragm
The diaphragm separates the thoracic and abdominal cavities. Defecating, urination, and even childbirth involve cooperation between the diaphragm and abdominal muscles (this cooperation is referred to as the “Valsalva maneuver”). While you hold your breath the diaphragm and abdominal muscles contract increasing the pressure of the peritoneal cavity and stabilizing the core. When the abdominal muscles contract, the pressure cannot push the diaphragm up, so it increases pressure on the intestinal tract (defecation), urinary tract (urination), or reproductive tract (childbirth).
The inferior surface of the pericardial sac and the inferior surfaces of the pleural membranes (parietal pleura) fuse onto the central tendon of the diaphragm. To the sides of the tendon are the skeletal muscle portions of the diaphragm, which insert into the tendon while having a number of origins including the xiphoid process of the sternum anteriorly, the inferior six ribs and their cartilages laterally, and the lumbar vertebrae and 12th ribs posteriorly.
The diaphragm also includes three openings for the passage of structures between the thorax and the abdomen. The inferior vena cava passes through the caval opening, and the esophagus and attached nerves pass through the esophageal hiatus. The aorta, thoracic duct, and azygous vein pass through the aortic hiatus of the posterior diaphragm.
Intercostal Muscles
There are three sets of muscles, called intercostal muscles, which span each of the intercostal spaces. The principal role of the intercostal muscles is to assist in breathing by changing the dimensions of the rib cage. The 11 pairs of superficial external intercostal muscles aid in inspiration of air during breathing because when they contract, they raise the rib cage, which expands it. The 11 pairs of internal intercostal muscles, just under the externals, are used for expiration because they draw the ribs together to constrict the rib cage. The innermost intercostal muscles are the deepest, and they act as synergists for the action of the internal intercostals.
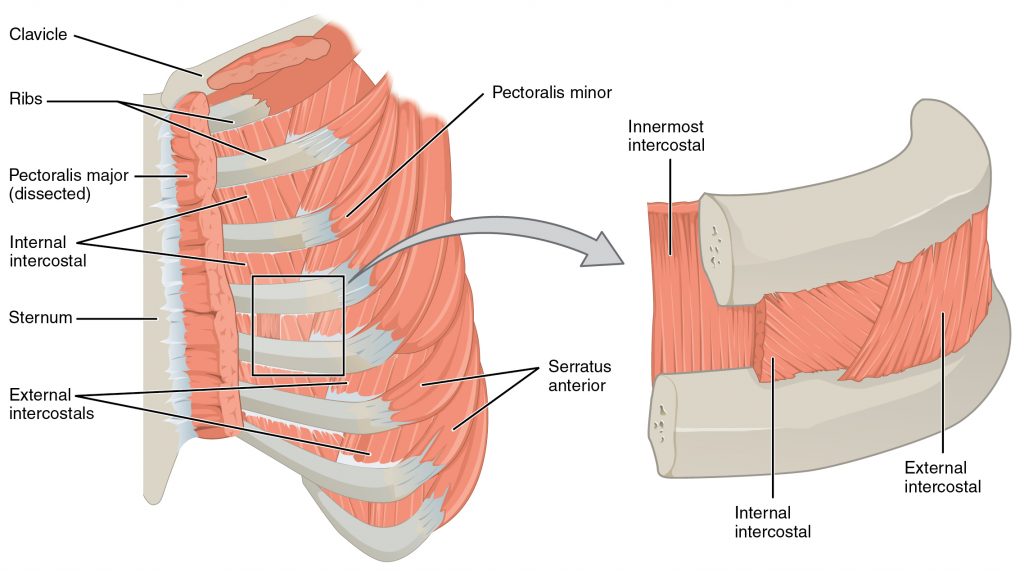
Intercostal Muscles.
The external intercostals are located laterally on the sides of the body. The internal intercostals are located medially near the sternum. The innermost intercostals are located deep to both the internal and external intercostals.
| Muscle | Origin | Insertion | Action | Innervation |
| Diaphragm | Cartilages of ribs 4-10, anterior surfaces of lumbar vertebrae & xyphoid process | Central tendinous sheet | Contracts to expand thoracic cavity | Phrenic nerve (C3-C5) |
| External intercostals | Inferior border of each rib/intercostal muscle | Superior border of each rib/intercostal muscle | Elevates ribs/ Elevation (expands thoracic cavity) | Intercostal nerves/branches of thoracic nerves |
| Internal intercostals | Superior border of each rib/intercostal muscles | Inferior border of each rib/intercostal muscle | Depress ribs, Movement along superior/inferior axis to bring ribs closer together | Intercostal nerves/branches of thoracic nerves |
| Transversus thoracis | Sternum/posterior surface | Rib cartilages | Depress ribs | Intercostal nerves/branches of thoracic nerves |
In The Lab
- Review the muscles of the thorax in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle with your lab partners.
Appendicular Muscles: Pectoral Girdle & Upper Limb
Objectives
- Locate the muscles of the pectoral girdle & upper limb on laboratory charts and models.
- Recognize on the models the origin, insertion, and action of the muscles of the pectoral girdle & upper limb.
- Describe and demonstrate the action of the muscles of the pectoral girdle & upper limb.
Muscles of the shoulder and upper limb can be divided into four groups: muscles that stabilize and position the pectoral girdle, muscles that move the arm, muscles that move the forearm, and muscles that move the wrists, hands, and fingers.
Muscles That Position the Pectoral Girdle
The pectoral girdle, or shoulder girdle, consists of the lateral ends of the clavicle and scapula, along with the proximal end of the humerus, and the muscles covering these three bones to stabilize the shoulder joint. The girdle creates a base from which the head of the humerus, in its ball-and-socket joint with the glenoid fossa of the scapula, can move the arm in multiple directions. Muscles that position the pectoral girdle are located either on the anterior thorax or on the posterior thorax. The anterior muscles include the subclavius, pectoralis minor, and serratus anterior. The posterior muscles include the trapezius, rhomboid major, and rhomboid minor. When the rhomboids are contracted, your scapula moves medially, which can pull the shoulder and upper limb posteriorly.
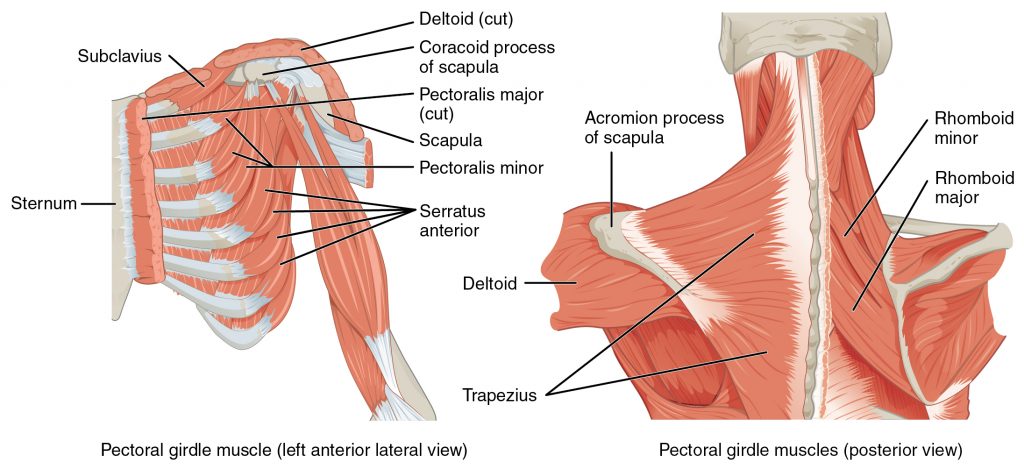
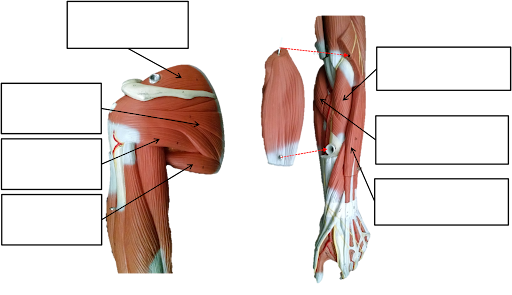
Muscles That Position the Pectoral Girdle.
The muscles that stabilize the pectoral girdle make it a steady base on which other muscles can move the arm. Note that the pectoralis major and deltoid, which move the humerus, are cut here to show the deeper positioning muscles.
| Muscles | Origin | Insertion | Action | Innervation |
| Serratus anterior | Superior & anterior margins of ribs 1-8/9 | Anterior surface of vertebral border of scapula | Rotates scapula for glenoid cavity to move upward, protracts shoulder | Long thoracic nerve (C 5-7) |
| Subclavius | Rib #1 | Inferior border of clavicle | Protracts & depresses shoulder | Subclavius nerve (C 5-6) |
| Trapezius | Spinous process of thoracic vertebrae, ligament nuchae, occipital bone | Scapular spine and acromion, clavicle | Extend neck
Elevate, retract, depress, rotate scapula, Elevate clavicle |
Accessory Nerve (N XI)
Cervical spinal nerves (C 3-4) |
| Pectoralis minor | Superior & anterior surface of rubs 3-5 | Scapula; coracoid process | Protracts/elevates shoulder
Rotates scapula to allow glenoid cavity to rotate downward |
Medial pectoral nerve ( C 8 ,T 1) |
| Rhomboid major | Spinous process of superior thoracic vertebrae | Scapula;vertebral border, from spine to inferior angle | Adducts scapula
Downward rotation of scapula |
Dorsal scapular nerve C 5 |
| Rhomboid minor | Spinous process of vertebrae C 7 – T 1 | Scapula;vertebral border | Adducts scapula
Downward rotation of scapula |
Dorsal scapular nerve C |
| Levator scapulae | Cervical vertebrae 1-4 (transverse processes)` | Scapula; vertebral border | Elevates scapula | Cervical nerves C 3 – 4 & dorsal scapular nerve;
C 5 |
In The Lab
- Review the muscles of the pectoral girdle in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle with your lab partners
Muscles That Move the Humerus
Similar to the muscles that position the pectoral girdle, muscles that cross the shoulder joint and move the humerus bone of the arm include both axial and scapular muscles. The two axial muscles are the pectoralis major and the latissimus dorsi. The pectoralis major is thick and fan-shaped, covering much of the superior portion of the anterior thorax. The broad, triangular latissimus dorsi is located on the inferior part of the back and has multiple points of origin including the lumbosacral fascia attached to the inferior 6 thoracic vertebrae, the inferior 3 ribs, the iliac crest and inferior angle of the scapula.
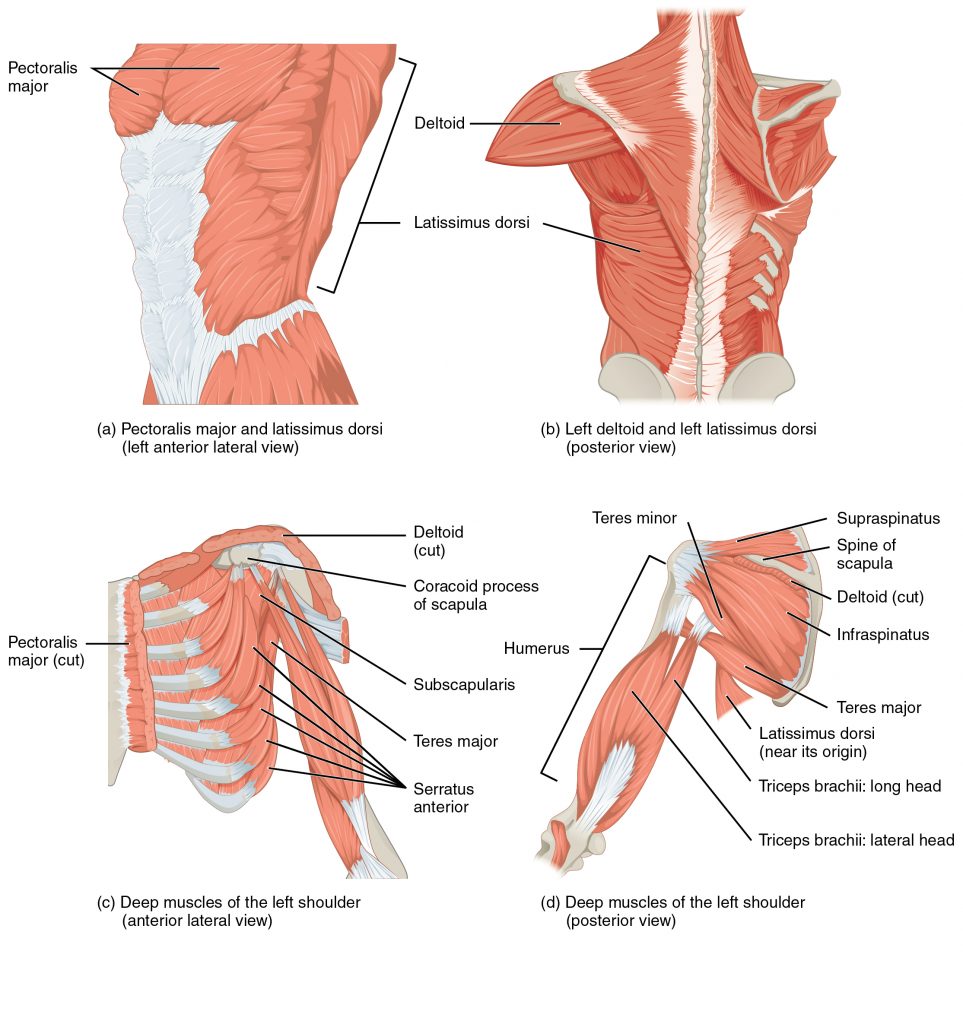
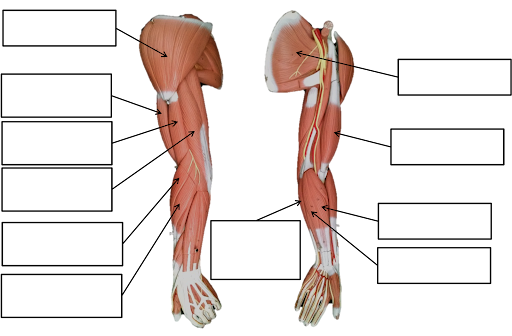
Muscles That Move the Humerus
(a, c) The muscles that move the humerus anteriorly are generally located on the anterior side of the body and originate from the sternum (e.g., pectoralis major) or the anterior side of the scapula (e.g., subscapularis). (b) The muscles that move the humerus superiorly generally originate from the superior surfaces of the scapula and/or the clavicle (e.g., deltoids). (c) The muscles that move the humerus inferiorly generally originate from middle or lower back (e.g., latissiumus dorsi). (d) The muscles that move the humerus posteriorly are generally located on the posterior side of the body and insert into the scapula (e.g., infraspinatus).
Axial muscles
| Muscle | Origin | Insertion | Action | Innervation |
| Pectoralis major | Clavicle; sternum; cartilage of certain ribs (1-6 or 1-7); aponeurosis of external oblique muscle | Greater tubercle of humerus | Adducts and medially rotates the arm | Lateral and medial pectoral nerve |
| Latissimus dorsi |
Thoracic vertebrae (T17-T12); lumbar vertebrae; lower ribs (9-12); iliac crest |
Intertubercular sulcus of humerus | Adducts the arm; Rotates the arm medially at the shoulder | Thoracodorsal nerve (C6-C8) |
Scapular muscles
| Muscle | Origin | Insertion | Action | Innervation |
| Deltoid |
Trapezius; clavicle; acromion; spine of scapula |
Nasal bone | Abducts the arm | Axillary nerve |
| Subscapularis | Subscapular fossa of scapula | Lesser tubercle of humerus | Medially rotates the arm; stabilizes shoulder joint during movement of the pectoral girdle | Upper and lower subscapular nerves |
| Supraspinatus | Supraspinous fossa of scapula | Greater tubercle of humerus | Abducts the arm; stabilizes shoulder joint | Suprascapular nerve |
| Infraspinatus | Infraspinous fossa of scapula | Greater tubercle of humerus | Rotates elbow laterally, as during a tennis swing | Suprascapular nerve |
| Teres major | Posterior surface of scapula | Intertubercular sulcus of humerus | Extends, medially rotates and adducts arm | Lower subscapular nerve |
| Teres minor | Lateral border of dorsal scapular surface | Greater tubercle of humerus | Rotates elbow laterally | Lower and upper subscapular nerve |
| Coracobra chialis | Coracoid process of scapula | Medial surface of humerus shaft | Flexes and adducts arm | Musculocutaneuous nerve |
The rest of the shoulder muscles originate on the scapula and help to move the arm. The deltoid is the major abductor of the arm but also facilitates flexing and medial rotation, as well as extension and lateral rotation. The subscapularis originates on subscapular fossa and medially rotates the arm. Named for their locations, the supraspinatus (originating from the supraspinous fossa) and the infraspinatus (originating from the infraspinous fossa) abduct the arm, and laterally rotate the arm, respectively. The thick and flat teres major is inferior to the teres minor and extends the arm, and assists in its adduction and medial rotation. The long teres minor laterally rotates the arm. Finally, the coracobrachialis flexes and adducts the arm.
The tendons of the subscapularis, supraspinatus, infraspinatus, and teres minor connect the scapula to the humerus, forming the rotator cuff (musculotendinous cuff), the circle of tendons around the shoulder joint. Although the shoulder joint allows a great deal of freedom of movement due to the shallow glenoid cavity it is extremely vulnerable to downward dislocation. The muscles and tendons of the rotator cuff provide stability to the joint. When baseball pitchers undergo shoulder surgery it is usually on the rotator cuff, which becomes pinched and inflamed, and may tear away from the bone due to the repetitive motion of bringing the arm overhead to throw a fast pitch.
Movements
- Flexion and extension of the shoulder joint in the (sagittal plane).
- Flexion is carried out by the anterior fibres of the deltoid, pectoralis major and the coracobrachialis.
- Extension is carried out by the latissimus dorsi and posterior fibres of the deltoid.
- Abduction and adduction of the shoulder (frontal plane).
- Abduction is carried out by the deltoid and the supraspinatus in the first 90 degrees.
- From 90-180 degrees it is the trapezius and the serratus anterior.
- Adduction is carried out by the pectoralis major, lattisimus dorsi, teres major and the subscapularis.
- Horizontal abduction and horizontal adduction of the shoulder (transverse plane)
- Medial and lateral rotation of shoulder (also known as internal and external rotation).
- Medial rotation is carried out by the anterior fibres of the deltoid, teres major, subscapularis, pectoralis major and the lattissimus dorsi.
- Lateral rotation is carried out by the posterior fibres of the deltoid, infraspinatus and the teres minor.
- Circumduction of the shoulder (a combination of flexion/extension and abduction/adduction).
Clinical Significance
The capsule can become inflamed and stiff, with abnormal bands of tissue (adhesions) growing between the joint surfaces, causing pain and restricting movement of the shoulder, a condition known as frozen shoulder or adhesive capsulitis.
A SLAP tear (superior labrum anterior to posterior) is a rupture in the glenoid labrum. SLAP tears are characterized by shoulder pain in specific positions, pain associated with overhead activities such as tennis or overhand throwing sports, and weakness of the shoulder. This type of injury often requires surgical repair.
Anterior dislocation of the glenohumeral joint occurs when the humeral head is displaced in the anterior direction. Anterior shoulder dislocation often is a result of a blow to the shoulder while the arm is in an abducted position. In younger people, these dislocation events are most commonly associated with fractures on the humerus and/or glenoid and can lead to recurrent instability. In older people, recurrent instability is rare but people often suffer rotator cuff tears.[citation needed] It is not uncommon for the arteries and nerves (axillary nerve) in the axillary region to be damaged as a result of a shoulder dislocation; which if left untreated can result in weakness, muscle atrophy, or paralysis.
Subacromial bursitis is a painful condition caused by inflammation which often presents a set of symptoms known as subacromial impingement.


Muscles of the Forearm
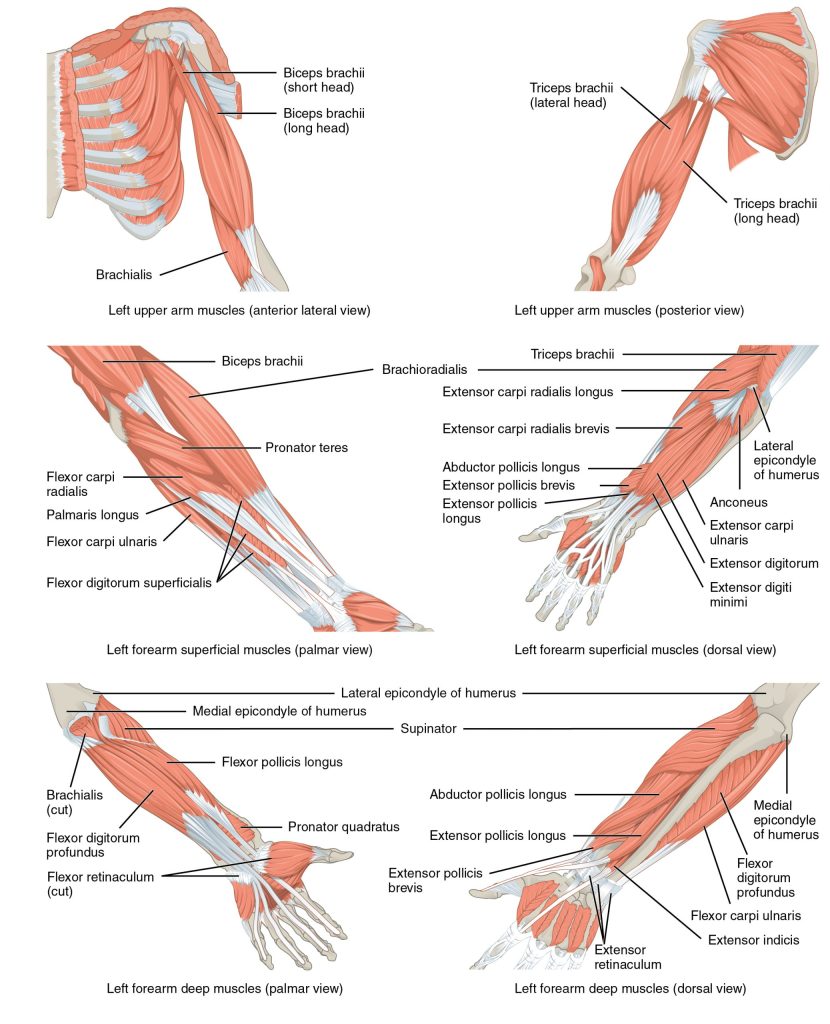
The forearm, made of the radius and ulna bones, has four main types of action at the hinge of the elbow joint: flexion, extension, pronation, and supination. When the forearm faces anteriorly, it is supinated. When the forearm faces posteriorly, it is pronated. The forearm flexors include the biceps brachii, brachialis, and brachioradialis. The extensors are the triceps brachii and anconeus. The pronators are the pronator teres and the pronator quadratus, and the supinator turns the forearm anteriorly.
The biceps brachii, brachialis, and brachioradialis flex the forearm. The two-headed biceps brachii crosses the shoulder and elbow joints to flex the forearm, also taking part in supinating the forearm at the radioulnar joints and flexing the arm at the shoulder joint. Deep to the biceps brachii, the brachial is a synergist in forearm flexion. Finally, the brachioradialis can flex the forearm quickly or help lift a load slowly. These muscles and their associated blood vessels and nerves form the anterior compartment of the arm (anterior flexor compartment of the arm)
Anterior muscles (flexion)
| Muscle | Origin | Insertion | Action | Innervation |
| Biceps brachii | Coracoid process; tubercle above glenoid cavity | Radial tuberosity | Flexes and supinates forearm | Musculocutaneous nerve |
| Brachialis |
Front of distal humerus |
Coronoid process of ulna | Flexes the elbrow | Musculocutaneous nerve; radial nerve |
| Brachioradialis | Lateral supracondylar ridge at distal end of humerus | Base of styloid process of radius | Flexes the forearm | Radial nerve |
Posterior muscles (extension)
| Muscle | Origin | Insertion | Action | Innervation |
| Triceps brachii | Infraglenoid tubercle of scapula; posterior shaft of humerus; posterior humeral shaft distal to radial groove | Olecranon process of ulna | Extends the forearm | Radial nerve |
| Anconeus | Lateral epicondyle of humerus | Lateral aspect of olecranon process of ulna | Extends elbow | Radial nerve |
Anterior muscles (pronation)
| Muscle | Origin | Insertion | Action | Innervation |
| Pronator teres | Medial epicondyle of humerus; coronoid process of ulna | Lateral radius | Pronates forearm | Median nerve |
| Pronator quadratus |
Distal portion of anterior ulnar shaft |
Distal surface of anterior radius | Assists in pronation forearm | Median nerve |
Posterior muscles (supination)
| Muscle | Origin | Insertion | Action | Innervation |
| Supinator | Lateral epicondyle of humerus; proximal ulna | Proximal end of radius | Supinates forearm | Posterior interosseous nerve |
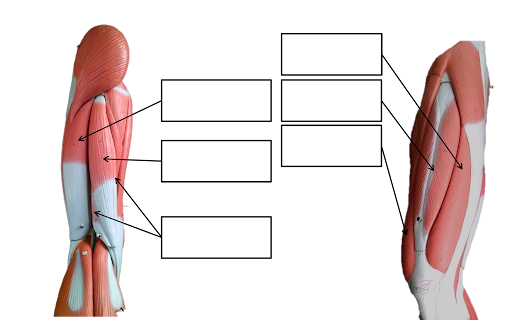
Muscles That Move the Forearm
The muscles originating in the upper arm flex, extend, pronate, and supinate the forearm. The muscles originating in the forearm move the wrists, hands, and fingers.
Muscles that Move the Hand, Wrist & Fingers
Wrist, hand, and finger movements are facilitated by two groups of muscles. The forearm is the origin of the extrinsic muscles of the hand. The palm is the origin of the intrinsic muscles of the hand.
Extrinsic Muscles of the Hand
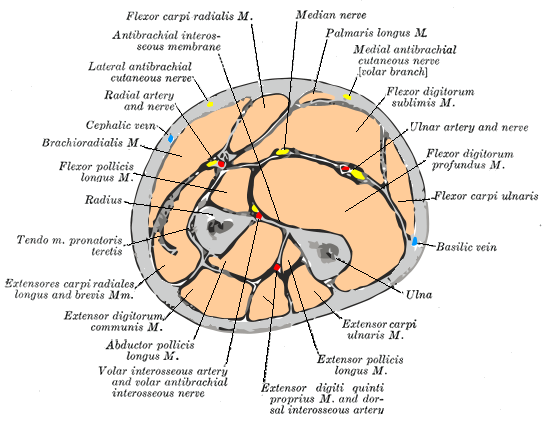
The muscles in the anterior compartment of the forearm (anterior flexor compartment of the forearm) originate on the humerus and insert onto different parts of the hand. These make up the bulk of the forearm. From lateral to medial, the superficial anterior compartment of the forearm includes the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and flexor digitorum superficialis. The flexor digitorum superficialis flexes the hand as well as the digits at the knuckles, which allows for rapid finger movements, as in typing or playing a musical instrument. However, repetitive movement with poor ergonomics can irritate the tendons of these muscles as they slide back and forth with the carpal tunnel of the anterior wrist and pinch the median nerve, which also travels through the tunnel, causing Carpal Tunnel Syndrome. The deep anterior compartment produces flexion and bends fingers to make a fist. These are the flexor pollicis longus and the flexor digitorum profundus.
The muscles in the superficial posterior compartment of the forearm (superficial posterior extensor compartment of the forearm) originate on the humerus. These are the extensor radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and the extensor carpi ulnaris.
The muscles of the deep posterior compartment of the forearm originate on the radius and ulna. These include the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis.
The tendons of the forearm muscles attach to the wrist and extend into the hand. Fibrous bands called retinacula sheath the tendons at the wrist. The flexor retinaculum extends over the palmar surface of the hand while the extensor retinaculum extends over the dorsal surface of the hand.
Superficial anterior compartment of forearm
| Muscle | Origin | Insertion | Action | Innervation |
| Flexor carpi radialis | Medial epicondyle of humerus | Base of second and third metacarpals | Flexes and abducts the hand | Median nerve |
| Palmaris longus | Medial epicondyle of humerus | Palmar aponeurosis; skin and fascia of palm | Tenses skin and fascia of palm. Aids in flexion of wrist and elbow | Median nerve |
| Flexor carpi ulnaris | Medial epicondyle of humerus; olecranon process; posterior surface of ulna | Pisiform, hamate bones, and base of fifth metacarpal | Flexes and abducts the hand | Ulnar nerve |
| Flexor digitorum superficialis | Medial epicondyle of humerus; coronoid process of ulna; shaft of radius | Middle phalanges of fingers 2-5 | Flexes wrist and middle phalanges of second to fifth fingers | Median nerve |
Deep anterior compartment of forearm
| Muscle | Origin | Insertion | Action | Innervation |
| Flexor pollicis longus | Anterior surface of radius; interosseous membrane | Distal phalanx of thumb | Flexes distal phalanx of thumb | Median nerve |
| Anconeus | Coronoid process; anteromedial surface of ulna; interosseous membrane | Distal phalanges of fingers 2-5 | Flexes distal interphalangeal joints | Median nerve; ulner nerve |
Superficial posterior compartment of forearm
| Muscle | Origin | Insertion | Action | Innervation |
| Extensor carpi radialis longus | Lateral supracondylar ridge of humerus | Base of second metacarpal | Extends and abducts the hand | Radial nerve |
| Extensor carpi radialis brevis | Lateral epicondyle of humerus | Base of third metacarpal | Extends and abducts the hand | Posterior interosseus nerve |
| Extensor digitorum | Lateral epicondyle of humerus | Extensor expansions; distal phalanges of fingers | Extends the hand and abducts the finger | Posterior interosseus nerve |
| Extensor digiti minimi | Lateral epicondyle of humerus | Extensor expansion; distal phalanx of finger 5 | Extends little finger | Posterior interosseus nerve |
| Extensor carpi ulnaris | Lateral epicondyle of humerus; posterior border of ulna | Base of fifth metacarpal | Extends and abducts the hand | Posterior interosseus nerve |
Deep posterior compartment of forearm
| Muscle | Origin | Insertion | Action | Innervation |
| Abductor pollicis longus | Posterior surface of radius and ulna; interosseous membrane | Base of first metacarpal; trapezium | Abducts and extends the thumb | Posterior interosseus nerve |
| Abductor pollicis longus | Dorsal shaft of radius and ulna; interosseous membrane | Base of proximal phalanx of thumb | Extends thumb | Posterior interosseus nerve |
| Abductor pollicis longus | Dorsal shaft of radius and ulna; interosseous membrane | Base of distal phalanx of thumb | Extends thumb | Posterior interosseus nerve |
| Extensor indicis | Posterior surface of distal ulna; interosseous membrane | Tendon of extensor digitorum of index finger | Extends index finger; aids in extending the wrist | Posterior interosseus nerve |
Muscles That Move the Wrist, Hands, and Forearm
Intrinsic Muscles of the Hand
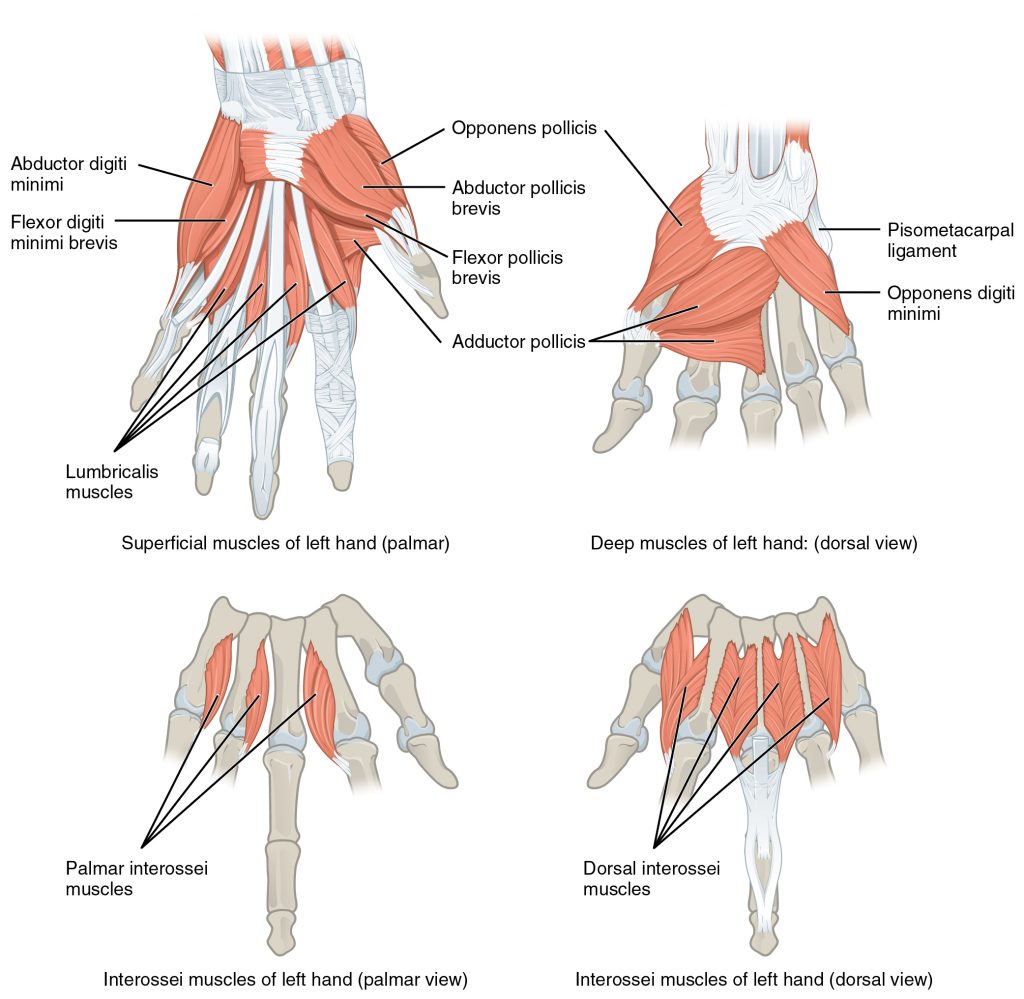
The intrinsic muscles of the hand both originate and insert within it. These muscles allow your fingers to make precise movements for actions, such as typing or writing. These muscles are divided into three groups. The thenar muscles are on the radial aspect of the palm. The hypothenar muscles are on the ulnar aspect of the palm, and the intermediate muscles are midpalmar.
The thenar muscles include the abductor pollicis brevis, opponens pollicis, flexor pollicis brevis, and the adductor pollicis. These muscles form the thenar eminence, the rounded contour of the base of the thumb, and all act on the thumb. The movements of the thumb play an integral role in most precise movements of the hand.
The hypothenar muscles include the abductor digiti minimi, flexor digiti minimi brevis, and the opponens digiti minimi. These muscles form the hypothenar eminence, the rounded contour of the little finger, and as such, they all act on the little finger. Finally, the intermediate muscles act on all the fingers and include the lumbrical, the palmar interossei, and the dorsal interossei.

Intrinsic Muscles of the Hand
The intrinsic muscles of the hand both originate and insert within the hand. These muscles provide the fine motor control of the fingers by flexing, extending, abducting, and adducting the more distal finger and thumb segments.
| Muscle | Origin | Insertion | Action | Innervation |
| Palmaris brevis | Aponeurosis of palmar | Medial border of hand skin | Medial border of skin moved to midline | Ulnar nerve, superficial branch C 8 |
| Adductor pollicis | Carpal & metacarpal bones | Thumb proximal phalanx | Adduction of thumb | Ulnar nerve, deep branch (C 8 – T 1) |
| Palmar interosseous (3-4) | Metacarpal bones (II, IV, V) | Proximal phalanges bases of fingers 2, 4, 5 | Adduction of metacarpophalangeal joints of 2, 4, 5.
Flexion at metacarpophalangeal joints. Extension at interphalangeal joints |
Ulnar nerve, deep branch (C 8 – T 1) |
| Abductor pollicis brevis | Transverse carpal ligament
Scaphoid, trapezium |
Base of proximal phalanx/thumb ; radial side | Abduction of thumb | Median nerve (C6 – C7) |
| Dorsal interosseous | Sides of metacarpals; originates from opposing faces of two metacarpal bones | Proximal phalanges of fingers 2-4 | Abduction at metacarpophalangeal joints of fingers 2&4.
Flexion at metacarpophalangeal joints. Extension at interphalangeal joints. |
Ulnar nerve, deep branch (C 8 – T 1) |
| Abductor digiti minimi | Pisiform | Little finger; proximal phalanx | Abduction & flexion of little finger. | Ulnar nerve, deep branch (C 8 – T 1) |
| Flexor pollicis brevis | Ulnar side of first metacarpal bone, flexor retinaculum, trapezium, capitate | Ulnar & radial sides of proximal phalanx of the thumb | Abduction & flexion of thumb | Branches of median & ulnar nerve |
| Flexor digiti minimi brevis | Hamate | Proximal phalanx of little finger | Little finger’ flexion of joints | Ulnar nerve, deep branch (C 8 – T 1) |
| Lumbricals | Tendons of flexor digitorum profundus | Digits 2-5; tendons of extensor digitorum | Digits; 2-5.
Extension at proximal & distal interphalangeal joints. |
Lumbricals 1 & 2; median nerve.
Lumbricals 3 & 4; ulnar nerve (deep branch) |
| Opponens pollicis | Flexor retinaculum & trapezium | 1st metacarpal bone | Thumb opposition | Median nerve C 6 _ C7_ |
| Opponens digiti minimi | Flexor retinaculum & trapezium | 5th metacarpal bone | 5th metacarpal bone opposition | Ulnar nerve C8 – T1 |
In The Lab
- Review the muscles of the humerus/shoulder/forearm/hand/wrist/fingers in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle with your lab partners
Appendicular Muscles: Pelvic Girdle & Lower Limb
Objectives
- Locate the muscles of the pelvic girdle & lower limb on laboratory charts and models.
- Recognize on the models the origin, insertion, and action of the muscles of the pelvic girdle & lower limb
- Describe and demonstrate the action of the muscles of the pelvic girdle & lower limb.
The appendicular muscles of the lower body position and stabilize the pelvic girdle, which serves as a foundation for the lower limbs. Comparatively, there is much more movement at the pectoral girdle than at the pelvic girdle. There is very little movement of the pelvic girdle because of its connection with the sacrum at the base of the axial skeleton and because the deep acetabulum provides a stable point of articulation with the head of the femur. The pelvic girdle’s lack of range of motion allows it to stabilize and support the body. The body’s center of gravity is in the area of the pelvis. If the center of gravity were not to remain fixed, standing up would be difficult. Therefore, what the leg muscles lack in range of motion and versatility, they make up for in size and power, facilitating the body’s stabilization, posture, and movement.
Muscles of the Pelvic Floor and Perineum
The pelvic floor (also referred to as the pelvic diaphragm) is a muscular sheet that defines the inferior portion of the pelvic cavity. The pelvic floor extends anteriorly to posteriorly from the pubis to the coccyx and is comprised of the levator ani and the ischiococcygeus. Its openings include the anal canal and urethra, and the vagina in women.
The large levator ani consists of two skeletal muscles, the pubococcygeus and the iliococcygeus. The levator ani is considered the most important muscle of the pelvic floor because it supports the pelvic viscera. It resists the pressure produced by contraction of the abdominal muscles so that the pressure is applied to the colon to aid in defecation and to the uterus to aid in childbirth (assisted by the ischiococcygeus, which pulls the coccyx anteriorly). This muscle also creates skeletal muscle sphincters at the urethra and anus.
The perineum is the diamond-shaped space between the pubic symphysis (anteriorly), the coccyx (posteriorly), and the ischial tuberosities (laterally), lying just inferior to the pelvic diaphragm (levator ani and ischiococcygeus). Divided transversely into triangles, the anterior is the urogenital triangle, which includes the external genitals and the posterior is the anal triangle containing the anus. The perineum is also divided into superficial and deep layers with some of the muscles common to men and women. Women also have the compressor urethrae and the sphincter urethrovaginalis, which function to close the vagina. In men, the deep transverse perineal muscle plays a role in ejaculation.
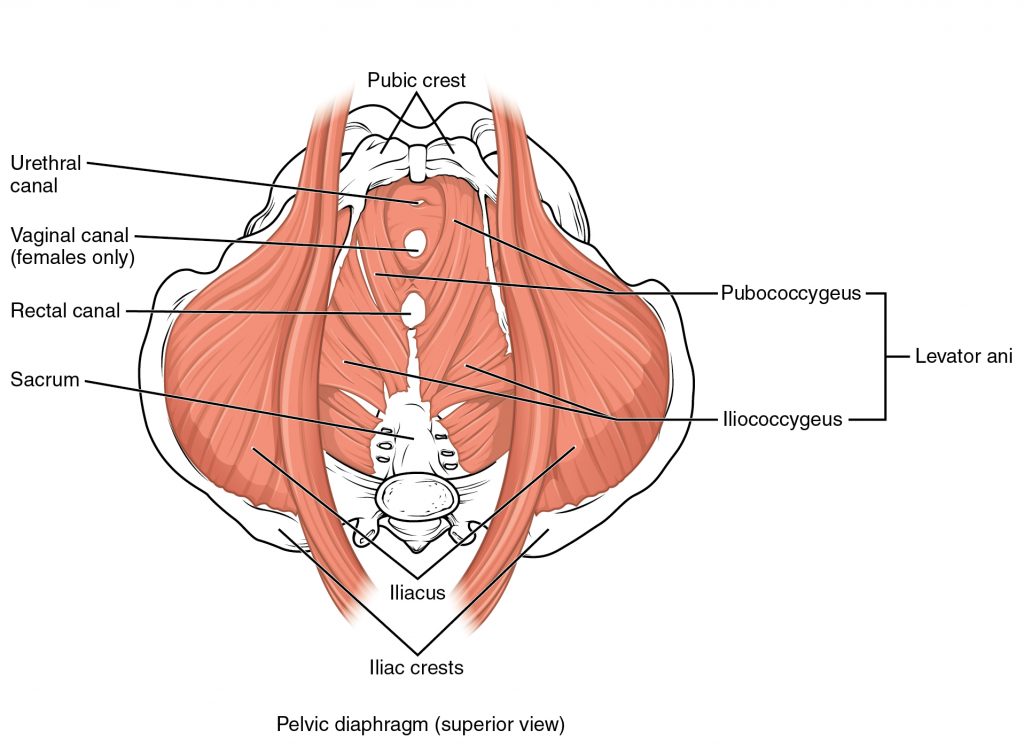
Muscles of the Pelvic Floor
The pelvic floor muscles support the pelvic organs, resist intra-abdominal pressure, and work as sphincters for the urethra, rectum, and vagina.
In The Lab
- Review the muscles of the pelvic floor & perineum in the images and tables provided
- Examine the pelvic floor & perineum muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each pelvic floor & perineum muscle using your and your lab partners.
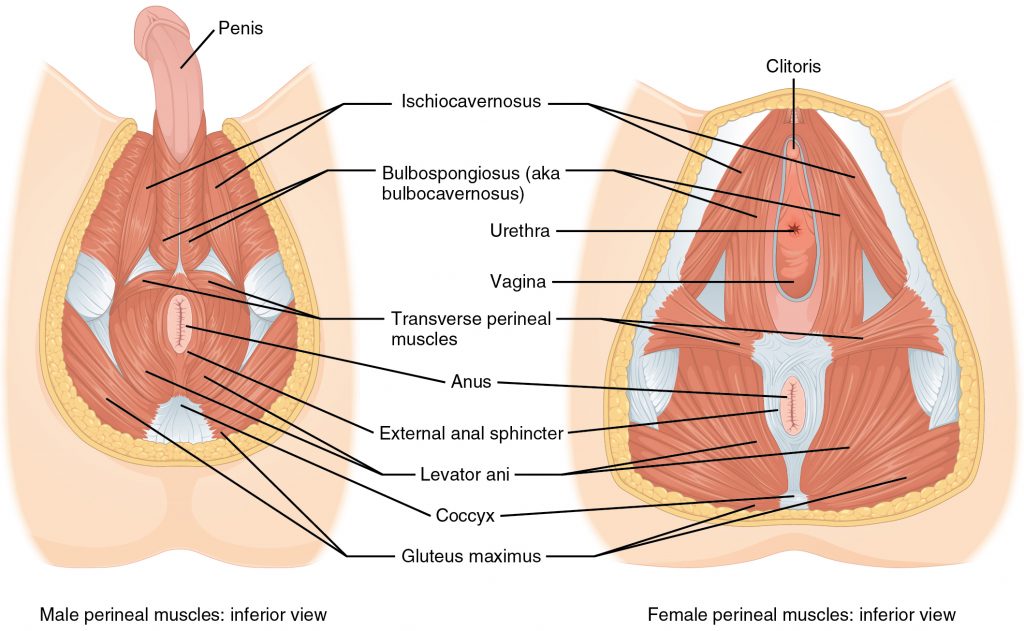
Muscles of the Perineum.
The perineum muscles play roles in urination in both sexes, ejaculation in men, and vaginal contraction in women.
Muscles of the Perineum Common to Men and Women
| Muscle | Origin | Insertion | Action | Innervation |
| Levator ani pubococcygeus; levator ani iliococcygeus | Pubis; Ischium | Urethra; anal canal; perineal body; coccyx | Compresses anal canal; Defecation; urination; birth; coughing | Pudendal nerve; Spinal nerves S2-S3 |
Superficial muscles
| Muscle | Origin | Insertion | Action | Innervation |
| Flexor pollicis longus | Anterior surface of radius; interosseous membrane | Distal phalanx of thumb | Flexes distal phalanx of thumb | Median nerve |
| Bulbospongiosus | Perineal body | Perineal body membrane; corpus spongiosum of penis; deep fascia of penis; clitoris in female | Involuntary response that compresses urethra when excreting urine in both sexes or while ejaculating in male; also aids in erection of penis in males | Pudendal nerve |
| Ischiocavernosus | Ischium; ischial rami; pubic rami | Pubic symphysis; corpus cavernosum of penis in male; clitoris of female | Compresses veins to maintain erection of penis in males; erection of clitoris in females | Pudendal nerve |
Deep muscles
| Muscle | Origin | Insertion | Action | Innervation |
| External urethral sphincter | Ischial rami; pubic rami | Male: median raphe; female: vaginal wall | Voluntarily compresses urethra during urination | Pedendal nerve spinal nerves S2-S4; pelvic splanchnic nerve |
| External anal sphincter | Anoccoccygeal ligament | Perineal body | Closes anus | Pedendal nerve spinal nerves S2-S4; pelvic splanchnic nerve |
Appendicular Muscles Of The Pelvic Girdle And Lower Limbs
The appendicular muscles of the lower body position and stabilize the pelvic girdle, which serves as a foundation for the lower limbs. Comparatively, there is much more movement at the pectoral girdle than at the pelvic girdle. There is very little movement of the pelvic girdle because of its connection with the sacrum at the base of the axial skeleton and because the deep acetabulum provides a stable point of articulation with the head of the femur. The pelvic girdle’s lack of range of motion allows it to stabilize and support the body. The body’s center of gravity is in the area of the pelvis. If the center of gravity were not to remain fixed, standing up would be difficult. Therefore, what the leg muscles lack in range of motion and versatility, they make up for in size and power, facilitating the body’s stabilization, posture, and movement.
Gluteal Region Muscles That Move the Thigh
Most muscles that insert on the femur (the thigh bone) and move it, originate on the pelvic girdle. The major flexors of the hip are the psoas major and iliac which make up the iliopsoas group. Some of the largest and most powerful muscles in the body are the gluteal muscles or gluteal group. The gluteus maximus, one of the major extensors of the thigh at the hip, is the largest; deep to the gluteus maximus is the gluteus medius, and deep to the gluteus medius is the gluteus minimus, the smallest of the trio.
The tensor fascia latae is a thick, squarish muscle in the superior aspect of the lateral thigh. It acts as a synergist of the gluteus medius and iliopsoas in flexing and abducting the thigh. It also helps stabilize the lateral aspect of the knee by pulling on the iliotibial tract (band), making it taut. Deep to the gluteus maximus, the piriformis, obturator internus, obturator externus, superior gemellus, inferior gemellus, and quadratus femoris laterally rotate the thigh at the hip.
Deep fascia in the thigh separates it into medial, anterior, and posterior compartments. The muscles in the medial compartment of the thigh responsible for adducting the femur at the hip are the adductor group including the adductor longus, adductor brevis, and adductor magnus which all adduct and medially rotate the thigh. The adductor longus also flexes the thigh, whereas the adductor magnus extends it. Like the adductor longs, the pectineus adducts and flexes the femur at the hip. The pectineus is located in the femoral triangle, which is formed at the junction between the hip and the leg and includes the femoral nerve, the femoral artery, the femoral vein, and the deep inguinal lymph nodes. The strap-like gracilis adducts the thigh in addition to flexing the leg at the knee.
The muscles of the anterior compartment of the thigh flex the thigh and extend the leg. This compartment contains the quadriceps femoris group, which is comprised of four muscles that extend the leg and stabilize the knee. Within the compartment the rectus femoris is on the anterior aspect of the thigh, the vastus lateralis is on the lateral aspect of the thigh, the vastus medialis is on the medial aspect of the thigh, and the vastus intermedius is between the vastus lateralis and vastus medialis and deep to the rectus femoris. The tendon common to all four is the quadriceps tendon (patellar tendon), which inserts into the patella and continues below it as the patellar ligament. The patellar ligament attaches to the tibial tuberosity. In addition to the quadriceps femoris, the sartorius is a band-like muscle that extends from the anterior superior iliac spine to the medial side of the proximal tibia. This versatile muscle flexes the leg at the knee and flexes, abducts, and laterally rotates the thigh at the hip. This muscle allows us to sit cross-legged.
The posterior compartment of the thigh includes muscles that flex the leg and extend the thigh. The three long muscles on the back of the thigh are the hamstring group, which flexes the knee. These are the biceps femoris, semitendinosus, and semimembranosus. The tendons of these muscles form the upper border of the popliteal fossa, the diamond-shaped space at the back of the knee.
In The Lab
- Review the muscles of muscles of the pelvic girdle in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle using yours and your lab partners.
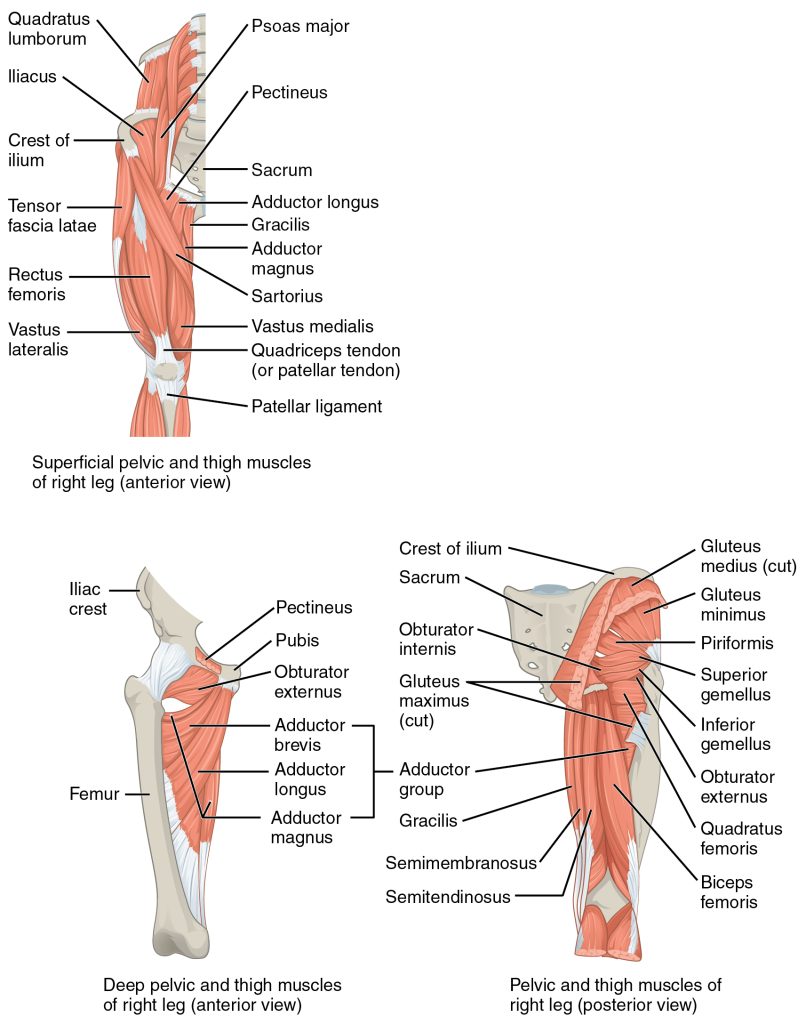
Hip and Thigh Muscles
The large and powerful muscles of the hip that move the femur generally originate on the pelvic girdle and insert into the femur. The muscles that move the lower leg typically originate on the femur and insert into the bones of the knee joint. The anterior muscles of the femur extend the lower leg but also aid in flexing the thigh. The posterior muscles of the femur flex the lower leg but also aid in extending the thigh. A combination of gluteal and thigh muscles also adduct, abduct, and rotate the thigh and lower leg.
Gluteal Region Muscles That Move the Femur
Iliopsoas group
| Muscle | Origin | Insertion | Action | Innervation |
| Psoas major | Lumbar verlebrae (L1-L5); thoracic vertebra (T1 2) | Lesser trochanter of femur | Flexes the thigh and vertebral column laterally | Anterior rami of lumbar spinal nerves |
| lliacus | Iliac fossa: iliac crest; lateral sacrum | Lesser trochanter of femur | Flexes the trunk and thigh | Femoral nerve |
Gluteal group
| Muscle | Origin | Insertion | Action | Innervation |
| Gluteus maximus | Dorsal ilium; sacrum; coccyx | Gluteal tuberosity of femur; Iliotibial tract | Extends the thigh | Inferior gluteal nerve |
| Gluteus medius | Lateral surface of ilium | Greater trochanter of femur | Abducts and medially rotates thigh | Superior gluleal nerve |
| Gluteus minimus | External surface of ilium | Greater trochanter of femur | Abducts and medially rotates thigh | Superior gluleal nerve |
| Tensor fascia lata | Anterior aspect of iliac crest; anterior superior iliac spine | Iliotibial tract | Steadies leg and trunk; rotates thigh medially; maintains posture by stabilizing the iliotibal track, which connects to the knee | Superior gluleal nerve |
Lateral rotators
| Muscle | Origin | Insertion | Action | Innervation |
| Piriformis | Anterolateral surface of sacrum | Greater trochanter of femur | Rotates extended thigh laterally; Slabilizes hip joint; Aids in abduction of thigh | Spinal nerves L5-S2 |
| Obutrator internus | Inner surface of obturator membrane; greater sciatic notch; margins of obturator foramen | Greater trochanter in front of piriformis | Rotates extended thigh laterally; Stabilizes hip joint; Aids in abduction of thigh | Nerve lo obturator infernus |
| Obturator externus | Outer surfaces of obturator membrane, pubic, and ischium; margins of obturator foramen | Trochanteric fossa of posterior femur | Rotates extended thigh laterally; Stabilizes hip joint; Aids in abduction of thigh | Obturator nerve |
| Superior gemellus | lschial spine | Greater trochanter of femur | Rotates extended thigh laterally; Stabilizes hip joint; Aids in abduction of thigh | Nerve lo obturator infernus |
| Inferior gemellus | Ischial tuberosity | Greater trochanter of femur | Rotates extended thigh laterally; Stabilizes hip joint; Aids in abduction of thigh | Nerve to quadratus femoris |
| Quadratus femoris | Ischial tuberosity | Trochanteric crest of femur | Extends and stabilizes leg; flexes thigh at hip | Nerve to quadratus femoris |
Adductors
| Muscle | Origin | Insertion | Action | Innervation |
| Adductor longus | Pubis near pubic symphysis | Linea aspera | Adducts, flexes and medially rotates thigh | Obturator nerve |
| External anal sphincter | Body of pubis; inferior ramus of pubis | Linea aspera above adductor longus | Adducts, flexes and medially rotates thigh | Obturator nerve |
| Adductor magnus | lschial rami; pubic rami; lschial tuberosity | Linea aspera; adductor tubercle of femur | Adducts and medially rotates flexes thigh. Aids in thigh extension | Obturator nerve; tibial nerve |
| Pectineus | Pedineal line of pubis | Lesser trochanter to linea aspera of posterior aspect of femur | Adducts thigh, flexes and medially rotates leg | Femoral nerve |
Muscles That Move the Feet and Toes
Similar to the thigh muscles, the muscles of the leg are divided by deep fascia into compartments, although the leg has three: anterior, lateral, and posterior.
The muscles in the anterior compartment of the leg all contribute to dorsiflexion: the tibialis anterior, a long and thick muscle on the lateral surface of the tibia, the extensor hallucis longus, deep under it, and the extensor digitorum longus, lateral to it. The fibularis tertius, a small muscle that originates on the anterior surface of the fibula, is associated with the extensor digitorum longus and sometimes fused to it, but is not present in all people. Thick bands of connective tissue called the superior extensor retinaculum (transverse ligament of the ankle) and the inferior extensor retinaculum, hold the tendons of these muscles in place during dorsiflexion.
The lateral compartment of the leg includes two muscles which contribute to eversion and plantar flexion: the fibularis longus (peroneus longus) and the fibularis brevis (peroneus brevis). The superficial muscles in the posterior compartment of the leg all insert onto the calcaneal tendon (Achilles tendon), a strong tendon that inserts into the calcaneal bone of the ankle, all contribute to plantar flexion. The muscles in this compartment are large and strong and keep humans upright. The most superficial and visible muscle of the calf is the gastrocnemius. Deep to the gastrocnemius is the wide, flat soleus. The plantaris runs obliquely between the two; some people may have two of these muscles, whereas no plantaris is observed in about seven percent of other cadaver dissections. The plantaris tendon is a desirable substitute for the fascia lata in hernia repair, tendon transplants, and repair of ligaments. There are four deep muscles in the posterior compartment of the leg as well: the popliteus, flexor digitorum longus, flexor hallucis longus, and tibialis posterior all contribute to plantar flexion or inversion of the foot.
The foot also has intrinsic muscles, which originate and insert within it (similar to the intrinsic muscles of the hand). These muscles primarily provide support for the foot and its arch, and contribute to movements of the toes (Figure 6 and Figure 7). The principal support for the longitudinal arch of the foot is a deep fascia called plantar aponeurosis, which runs from the calcaneus bone to the toes (inflammation of this tissue is the cause of “plantar fasciitis,” which can affect runners. The intrinsic muscles of the foot include the extensor digitorum brevis on the dorsal aspect and a plantar group, which consists of four layers.

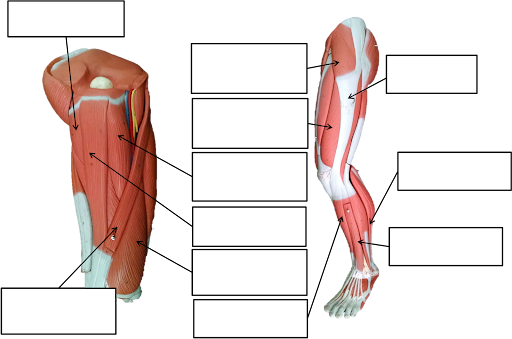
Muscles of the Lower Leg
The muscles of the anterior compartment of the lower leg are generally responsible for dorsiflexion, and the muscles of the posterior compartment of the lower leg are generally responsible for plantar flexion. The lateral and medial muscles in both compartments invert, evert, and rotate the foot.
Anterior compartment of leg
| Muscle | Origin | Insertion | Action | Innervation |
| Tibialis anterior | Lateral condyle and upper tibial shaft; interosseous membrane | Interior surface of medial cuneiform; First metatarsal bone | Dorsiflexes the foot; inverts foot; aids in support of medial longitudinal arch of foot | Deep fibular (peroneal) nerve |
| Extensor hallucis longus | Anteromedial fibula shaft; interosseous membrane | Distal phalanx of big toe | Extends big toe; aids in dorsiflexion of the foot | Deep fibular (peroneal) nerve |
| Extensor digitorum longus | Lateral condyle of tibia; proximal portion of fibula; interosseous membrane | Middle and distal phalanges of toes 2-5 | Extends toes; dorsiflexes the foot | Deep fibular (peroneal) nerve |
Lateral compartment of leg
| Muscle | Origin | Insertion | Action | Innervation |
| Fibularis longus | Upper portion of lateral fibula | First metatarsal medial cuneiform | Plantar Rexes and everts foot | Superficial fibular (peroneal) nerve |
| Fibularis (peroneus) brevis | Distal fibula shaft | Proximal end of fifth metatarsal | Plantar Rexes and everts foot | Superficial fibular (peroneal) nerve |
Posterior compartment of leg: Superficial muscles
| Muscle | Origin | Insertion | Action | Innervation |
| Gastrocnemius | Medial and lateral condyles of femur | Posterior calcaneus | Plantar flexes the foot; flexes knee when foot is dorsiflexed | Tibial nerve |
| Soleus | Superior tibia; fibula; interosseous membrane | Posterior calcaneus | Plantar flexes foot | Tibial nerve |
| Plantaris | Posterior femur above lateral condyle | Calcaneus or calcaneus tendon | Aids in flexing the leg and plantar flexing the foot | Tibial nerve from anterior rami of S1-S2 |
| Tibialis posterior | Superior tibia and fibula; interosseous membrane | Several tarsals and metatarsals 2-4 | Inverts and plantar flexes foot; aids in stabilizing medial longitudinal arch of foot | Tibial nerve |
Posterior compartment of leg: Deep muscle
| Muscle | Origin | Insertion | Action | Innervation |
| Poplileus | Lateral condyle of femur; lateral meniscus | Proximal tibia | Flexes and rotates leg medially to unlock extended knee when flexion begins; laterally rotates thigh | Tibial nerve |
| Flexor digitorum longus | Posterior tibia | Distal phalanges of toes 2-5 | Plantar flexes and inverts foot; flexes toes | Tibial nerve |
| Flexor hallucis longus | Midshaft of fibula; interosseous membrane | Distal phalanx of big, toe | Plantar flexes and inverts foot; flexes toes | Tibial nerve |
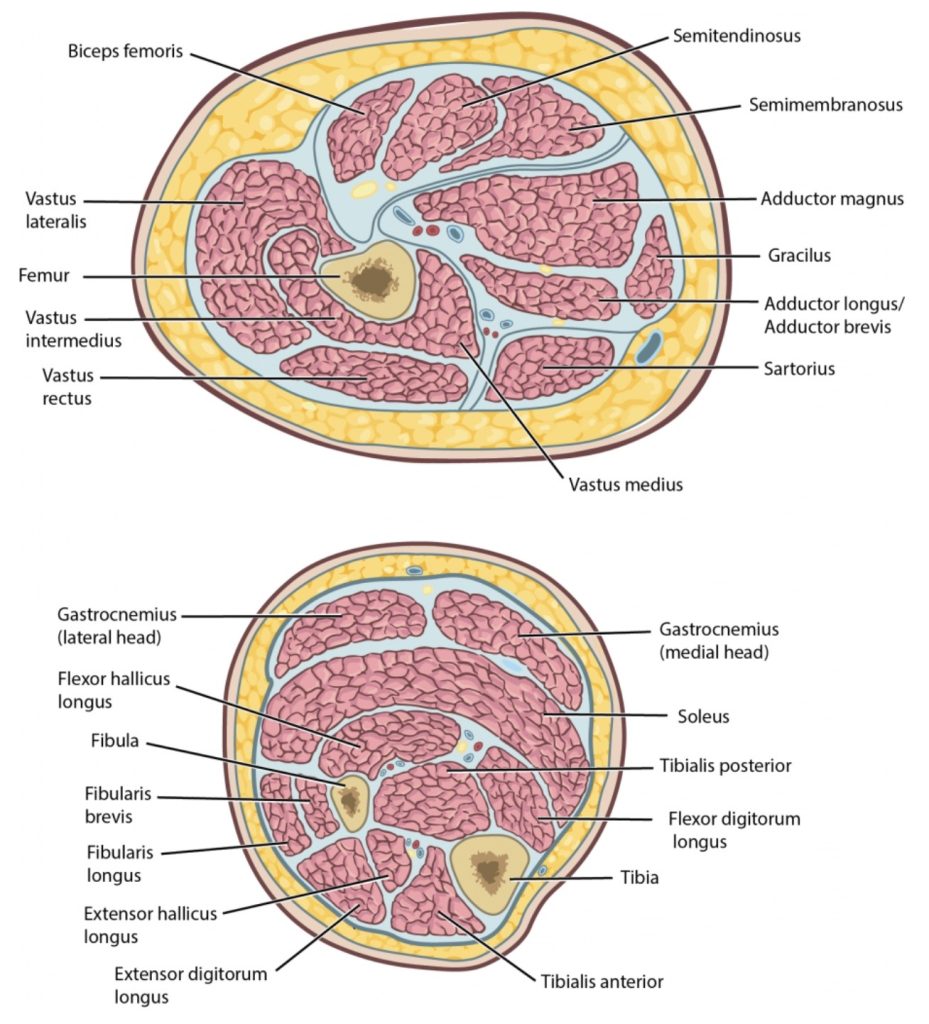
Compartments of the leg.
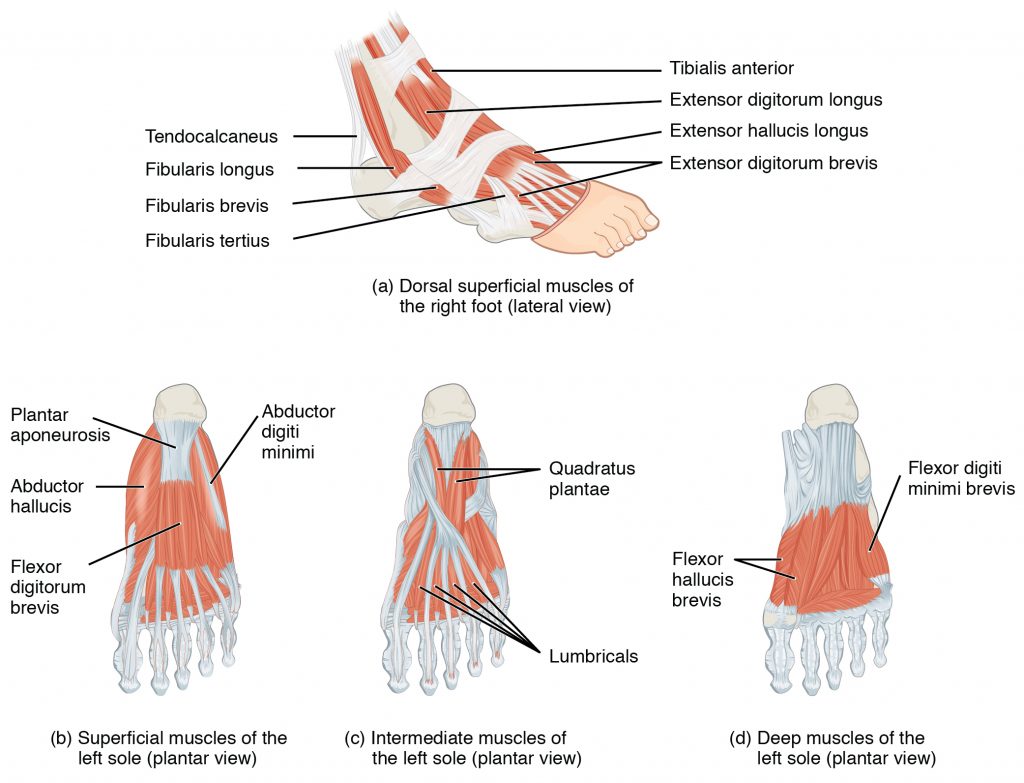
Intrinsic Muscles of the Foot
The muscles along the dorsal side of the foot (a) generally extend the toes while the muscles of the plantar side of the foot (b, c, d) generally flex the toes. The plantar muscles exist in three layers, providing the foot the strength to counterbalance the weight of the body. In this diagram, these three layers are shown from a plantar view beginning with the bottom-most layer just under the plantar skin of the foot (b) and ending with the top-most layer (d) located just inferior to the foot and toe bones.
In The Lab
- Review the muscles of the lower limb in the images and tables provided
- Examine the model and muscles charts provided in lab, locate each muscle (origin, insertion & innervation) and describe its action.
- Review the movement and action of each muscle with your lab partners
Dorsal group
| Prime mover | Origin | Insertion | Action | Innervation |
| Extensor digitorum brevis | Calcaneus; extensor retinaculum | Base of proximal phalanx of big toe; extensor expansions on toes 2-5 | Extends toes 2-5 | Posterior interosseous nerve |
Plantar group (layer 1)
| Prime mover | Origin | Insertion | Action | Innervation |
| Abductor hallucis | CalcaneaJ tuberosity; flexor retinaculum | Proximal phalanx of big toe | Abducts and flexes big toe | Medial plantar nerve |
| Flexor digitorum brevis | Calcaneal tuberosity | Middl’e phalanx of toes 2-4 | Flexes toes 2-4 | Superficial branch of the lateral plantar nerve |
| Abductor digiti minimi | Calcaneal tuberosity | Proximal phalanx of little toe | Abducts and flexes small toe | superficial branch of the lateral plantar nerve |
Plantar group (layer 2)
| Prime mover | Origin | Insertion | Action | Innervation |
| Quadratus plantae | Medial and lateral sides of calcaneus | Tendon of flexor digitorum longus | Flexes and rotates leg medially to unlock extended knee when flexion begins; laterally rotates thigh | Lateral plantar nerve (S1-S2) |
| Lumbricals | Tendons of flexor digitorum longus | Medial side of proximal phalanx of toes 2-5 | Extends toes 2-5 at the interphalangeal joints; flexes the small toes at the metatarsophalangeal joints | Medial and lateral plantar nerves (S3) |
Plantar group (layer 3)
| Prime mover | Origin | Insertion | Action | Innervation |
| Flexer hallucis brevis | Lateral cuneiform; cuboid bones | Base of proximal phalanx of big toe | Flexes big toe | Medial plantar nerve |
| Adductor hallucis | Bases of metatarsals 2-4; fibular,is longus tendon sheath; ligament across metatarsophalangeal joints | Base of proximal phalanx of big toe | Adducts and flexes big toe | Lateral plantar nerve |
| Flexor digiti minimi brevis | Base of metatarsal 5; tendon sheath of fibularis longus | Base of proximal phalanx of little toe | Flexes small toe | Superficial branch of the lateral plantar nerve |
Plantar group (layer 4)
| Prime mover | Origin | Insertion | Action | Innervation |
| Dorsal interossei | Sides of metatarsals | Both sides of toe 2; for each other toe, extensor expansion over first phalanx on side opposite toe 2 | Abducts and flexes middle toes at metatarsophalangeal joints; extends middle toes at interphalangeal joints | Lateral plantar nerve |
| Plantar interossei | Sides of metatarsal that faces metatarsal 2 (absent from metatarsal 2) | Extensor expansion on first phalanx of each toe (except to 2) on side facing toe 2 | Abducts toes 3-5; flexes proximal phalangeal and extends distal phalanges | Lateral plantar nerve |
Intrinsic Muscles in the Foot
Laboratory Activity
- Muscle Terminology
Label the following:
B. Gross Anatomy of the Muscular System
Head & Neck
Torso – Anterior view

Torso posterior view
Arm
Torso and Leg
Leg
Leg
Leg
List of Muscles to Identify in the lab using Anatomical Models
Muscles of facial expression
| Name | Action | Origin | Insertion |
| Frontalis | Raises eyebrows, wrinkles forehead | Frontal Bone | Skin of the brow |
| Occipitalis | Pull scalp posteriorly | Occipital bone | Aponeurosis connecting to frontalis |
| Orbicularis oris | Closes mouth | Maxillae and Mandible | Lips |
| Zygomaticus (major/minor) | Smile | Zygomatic Bone | mouth |
| Orbicularis oculi | Closes eye | Margin of Orbit | Eyelid |
| Masseter | Elevates mandible | Zygomatic Arch | Mandible |
| Temporalis | Elevates mandible | Temporal Bone | Mandible |
| Buccinator | Presses cheek inward | Maxillae and Mandible | orbicularis oris |
Muscles of the head, vertebral column and abdominal wall
| Name | Action | Origin | Insertion |
| Splenius capitis | extend + laterally flex head | upper spine | Temporal & occipital |
| Sternocleidomastoid | Flexes + rotates neck (also elevates ribs) | Sternum & Clavicle | Mastoid Process |
| Scalenes | Flexes neck (also elevates ribs) | Cervical Vertebrae | 1st Two Ribs |
| Rectus abdominus | Flexes vertebral column , compresses abdomen | Pubis | Lower Ribs and Xiphoid |
| External oblique | Flexes + rotates vertebral column, compresses abdomen | Lower Ribs | Linea alba and Ilium |
| Internal oblique | Flexes + rotates vertebral column, compresses abdomen | Lumbar Vertebrae & Ilium | Lower Ribs, Linea alba, Sternum |
| Transverse abdominus | Compresses abdomen | Lower Ribs, Ilium, Lumbar Vertebrae | Linea Alba & Pubis |
| Erector spinae group | Extends vertebral column | Ilium, Sacrum, Ribs, Vertebrae | Ribs, Vertebrae, Base of Skull |
| Levator scapulae | Extends neck (also elevates scapula) | Cervical Vertebrae | Scapula |
Thoracic & shoulder muscles
| Name | Action | Origin | Insertion |
| Pectoralis major | Flexes, adducts + medially rotates arm at shoulder | Sternum & Clavicle | Humerus |
| Pectoralis minor | Elevates ribs (also moves scapula anterior and inferior) | Ribs | Scapula |
| External intercostals | Elevates ribs | Inferior Rib | Superior rib |
| Internal intercostals | Depresses ribs | Superior rib | Inferior Rib |
| Diaphragm | Increases thoracic volume | Xiphoid Process, Ribs, Lumbar Vertebrae | Central Tendinous Sheet |
Arm movers
| Name | Action | Origin | Insertion |
| Serratus anterior | Moves and fixes scapula anteriorly | Ribs | Scapula |
| Trapezius | Elevates, retracts, depresses+ rotates scapula upward (also extends neck) | Occipital Bone & Thoracic Vertebrae | Scapula |
| Rhomboids (major & minor) | Elevates + adducts scapula | Cervical & Thoracic Vertebrae | Scapula |
| Latissimus dorsi | Extends, adducts + medially rotates arm at shoulder | Thoracic, Lumbar Vertebrae, Ribs | Humerus |
| Deltoid | Abducts arm at shoulder (also anterior fibers flex + posterior fibers extend arm at shoulder) | Clavicle & Scapula | Humerus |
| Teres major | Medially rotate arm | Scapula | Humerus |
Rotator cuff
| Name | Action | Origin | Insertion |
| Infraspinatus | Laterally rotates shoulder | Scapula | Humerus |
| Supraspinatus | Abducts shoulder | Scapula | Humerus |
| Subscapularis | Medially rotates shoulder | Scapula | Humerus |
| Teres minor | Laterally rotates shoulder | Scapula | Humerus |
Forearm movers
| Name | Action | Origin | Insertion |
| Biceps brachii | Flexes arm at elbow | Scapula | Radius |
| Brachialis | Flexes arm at elbow | Humerus | Ulna |
| Triceps brachii | Extends arm at elbow | Humerus & Scapula | Ulna |
| Pronator teres | Pronates forearm | Humerus & Ulna | Radius |
| Supinator | Supinates forearm | Humerus & Ulna | Radius |
| Brachioradialis | Flexes arm at elbow (beer raising) | Humerus | Radius |
Hand & finger movers
| Name | Action | Origin | Insertion |
| Flexor carpi radialis | Flexes & abducts hand at wrist | Humerus | Carpal Bones |
| Palmaris longus | Flexes hand at wrist | Humerus | Carpal Bones |
| Flexor carpi ulnaris | Flexes & adducts hand at wrist | Humerus | Carpal Bones |
| Extensor carpi radialis | Extends & abducts hand at wrist | Humerus | Carpal Bones |
| Extensor digitorum | Extends fingers | Humerus | Digits |
| Extensor carpi ulnaris | Extends & adducts hand at wrist | Humerus | Carpal Bones |
Muscles of the thigh & leg
| Name | Action | Origin | Insertion |
| Flexor digitorum longus | Flexes toes | Tibia | Digits |
| Flexor hallucis longus | Flexes hallux | Fibula | big toe |
| Tibialis anterior | Dorsiflex foot at ankle, inverts foot | Tibia | 1st metatarsal |
| Extensor digitorum longus | Extends toes | Tibia & fibula | digits |
| Fibularis (peroneus) longus | plantarflexes | Tibia & fibula | 1st metatarsal |
| Gastrocnemius | plantarflexes | Femur | calcaneous |
| Soleus | Plantarflexes | Femur & tibia | calcaneous |
Muscles of the leg & thigh
| Name | Action | Origin | Insertion |
| Psoas major | Flexes thigh at hip and vertebral column | Thoracic and Lumbar Vertebrae | Femur |
| Iliacus | Flexes thigh at hip | Ilium | Femur |
| Adductor longus | Adducts thigh at hip | Pubis | Femur |
| Adductor magnus | Adducts thigh at hip | Pubis and Ischium | Femur |
| Gracilis | Adducts thigh at hip | Pubis | Tibia |
| Gluteus maximus | Extends thigh at hip, rotates thigh laterally | Ilium, Sacrum and Coccyx | Femur, ITB |
| Gluteus medius | Abducts thigh at hip, rotates thigh medially | Ilium | Femur |
| Sartorius | Flexes leg at knee (also flexes + rotates thigh at hip) | Ilium | Tibia |
| Tensor fascia latae | tenses the ITB, supports knee | Ilium | ITB |
Quadriceps femoris
| Name | Action | Origin | Insertion |
| Rectus femoris | Extends leg at knee (also flexes thigh at hip) | Ilium | Tibia |
| Vastus lateralis | Extends leg at knee | Femur | Tibia |
| Vastus medialis | Extends leg at knee | Femur | Tibia |
| Vastus intermedius | Extends leg at knee | Femur | Tibia |
Hamstrings
| Name | Action | Origin | Insertion |
| Biceps femoris | Flexes leg at knee (also extends thigh at hip) | Ischium & Femur | Tibia & Fibula |
| Semitendinosus | Flexes leg at knee (also extends thigh at hip) | Ischium | Tibia |
| Semimembranosus | Flexes leg at knee (also extends thigh at hip) | Ischium | Tibia |
Media Attributions
- Front and side views of facial expressions_Muscles © Wikipedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- Extrinsic eye muscles © By OpenStax - https://cnx.org/contents/FPtK1zmh@8.25:fEI3C8Ot@10/Preface, CC BY 4.0, https://commons.wikimedia.org/w/index.php?curid=30131681 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Extraocular actions and innervation © By Au.yousef - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=35019028 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles That Move the Lower Jaw © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles of the tongue © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscle of the anterior neck © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles of the neck and back © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles of the abdomen © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Diaphragm © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Thorax © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles that position the pectoral girdle © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles that move the humerus © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Shoulder joint © By Jmarchn - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=67117834 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Shoulder joint back © By Jmarchn - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=67117834
- middle of the forearm © By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See "Book" section below)Bartleby.com: Gray's Anatomy, Plate 417, Public Domain, https://commons.wikimedia.org/w/index.php?curid=3454672 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles that move the forearm © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Wrist and hand dissection
- Muscles of the hand © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Pelvic floor muscles © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Perineum muscles © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Hip and Thigh Muscles © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Muscles of the Lower Leg © Anatomy & Physiology by OpenStax is licensed under a CC BY-SA (Attribution ShareAlike) license
- Compartments of the leg © Maria Carles is licensed under a CC BY-SA (Attribution ShareAlike) license
- Intrinsic Muscles of the Foot © Anatomy & Physiology by OpenStax is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Label Muscle Terminology © LibreTexts is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Label Head & Neck © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Torso anterior view © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Torso posterior view © Torso posterior view is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Arm © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Arm 2 © Maria Carles is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Torso and Leg © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Leg © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Leg 2 © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license
- Label Leg 3 © LibreTexts is licensed under a CC BY-SA (Attribution ShareAlike) license

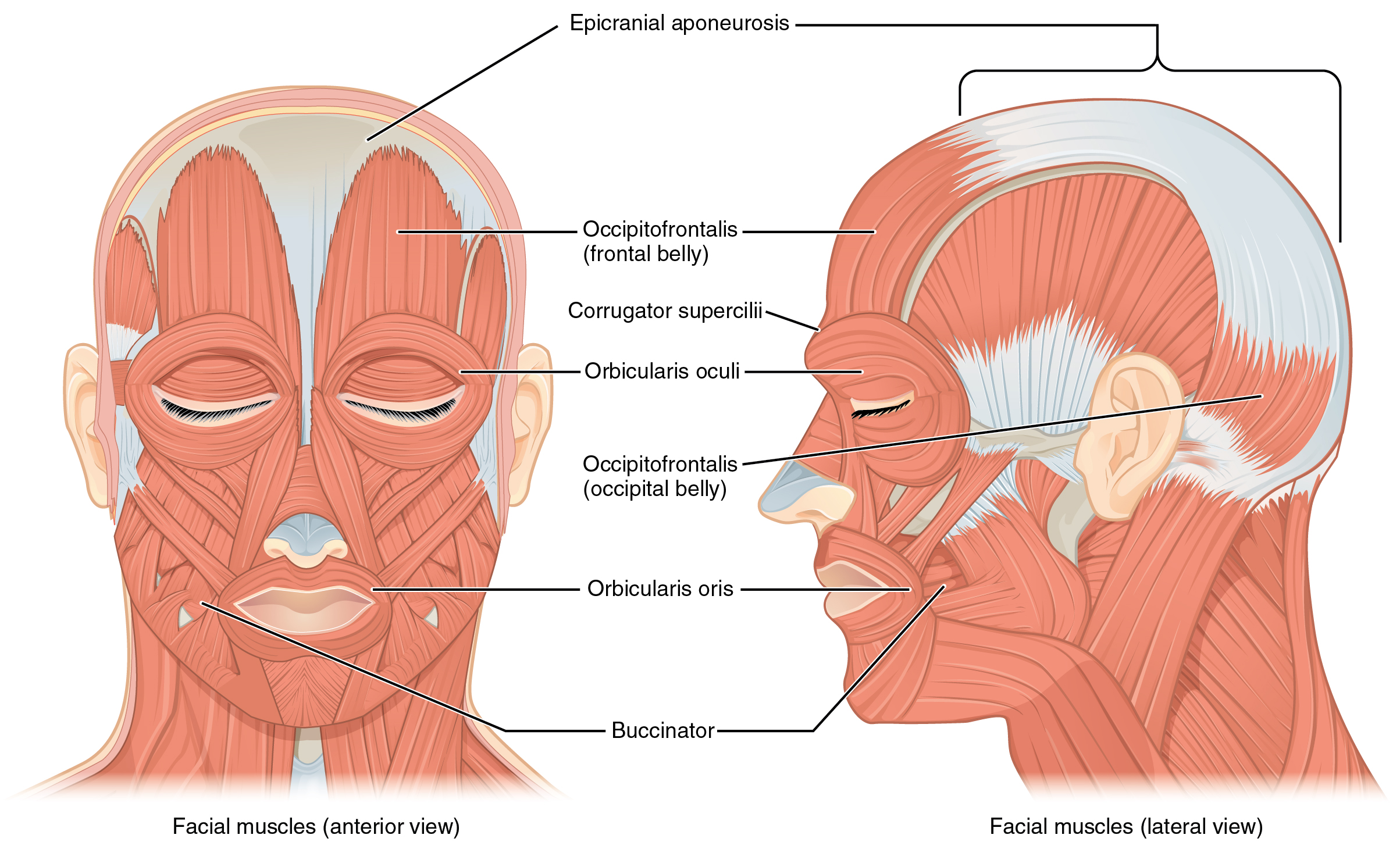{kind=link}
{kind=link}
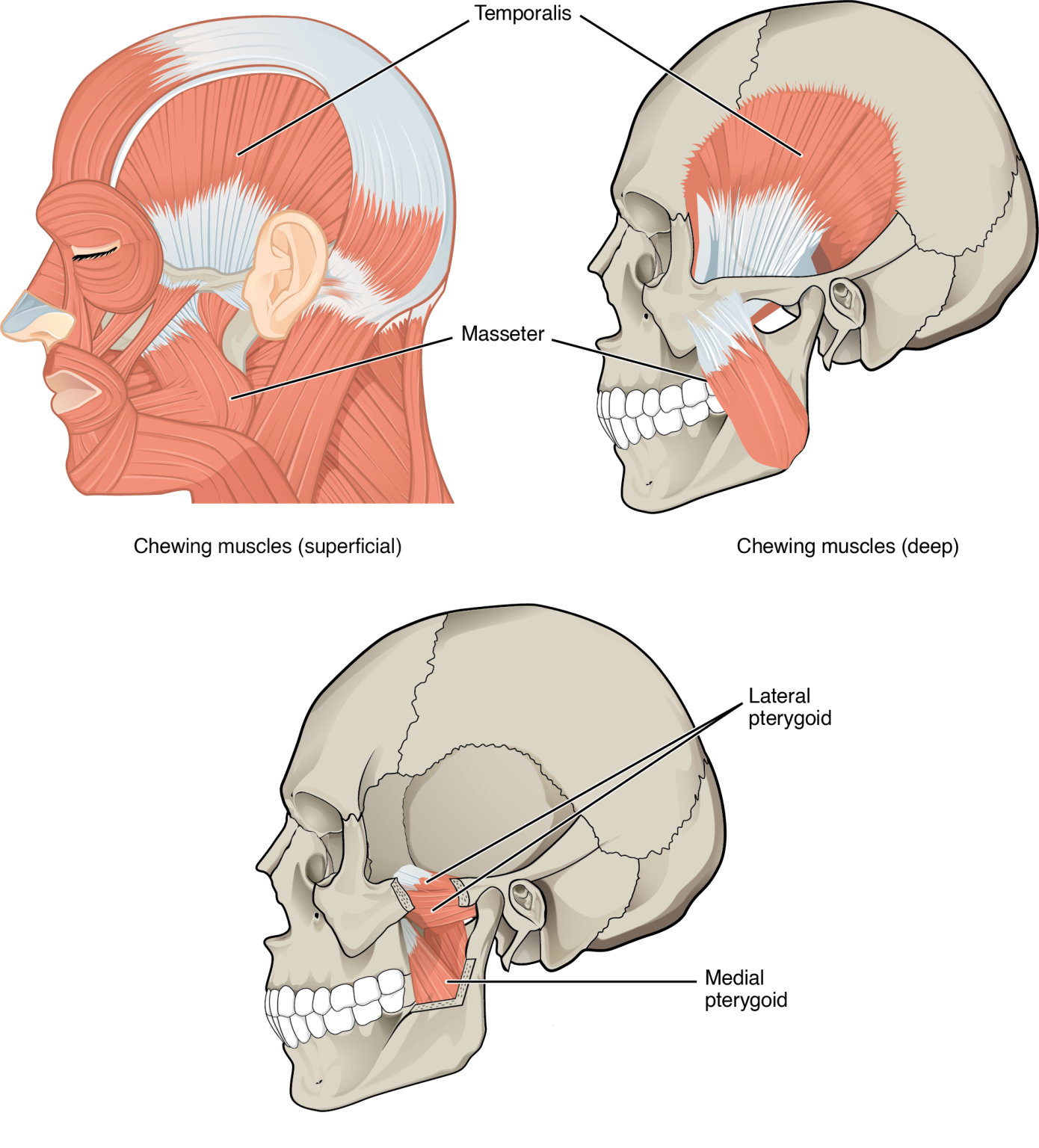{kind=link}
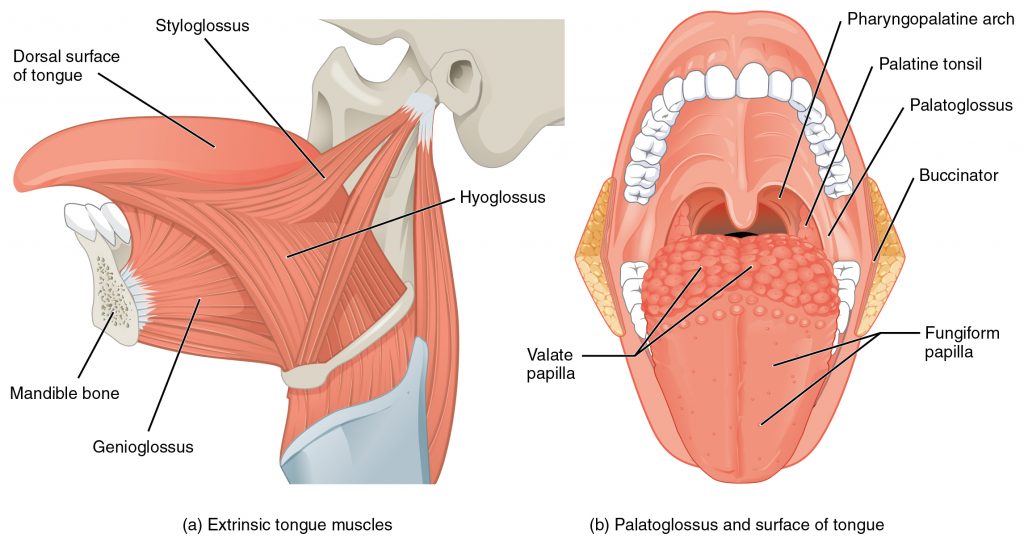{kind=link}
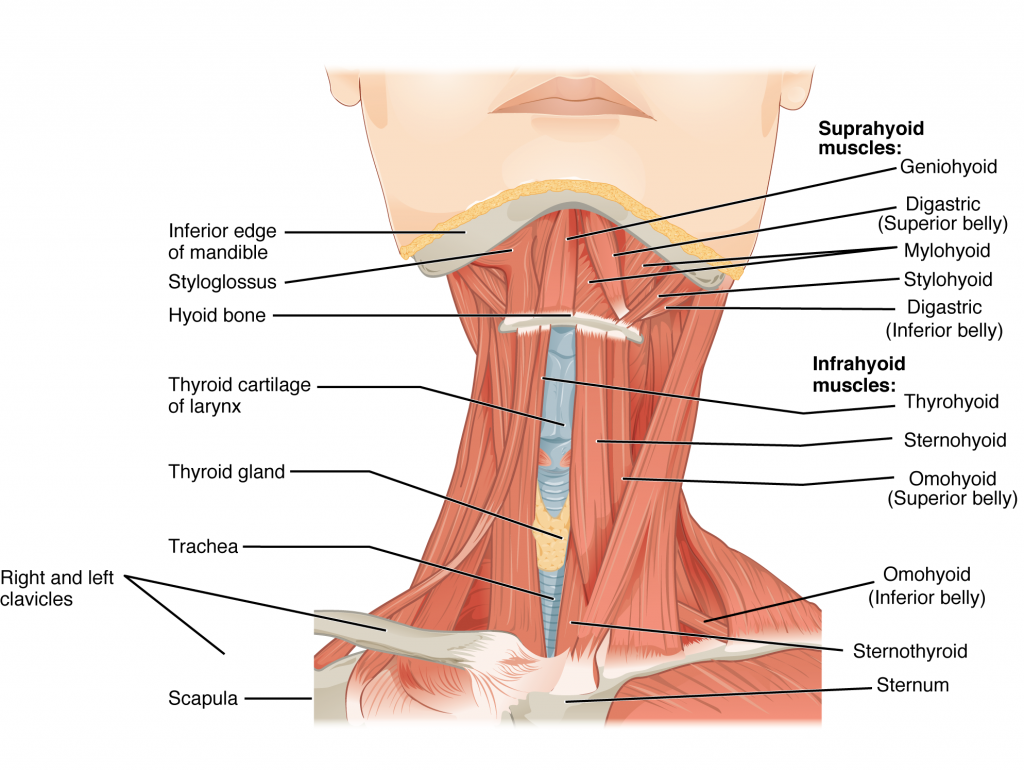{kind=link}
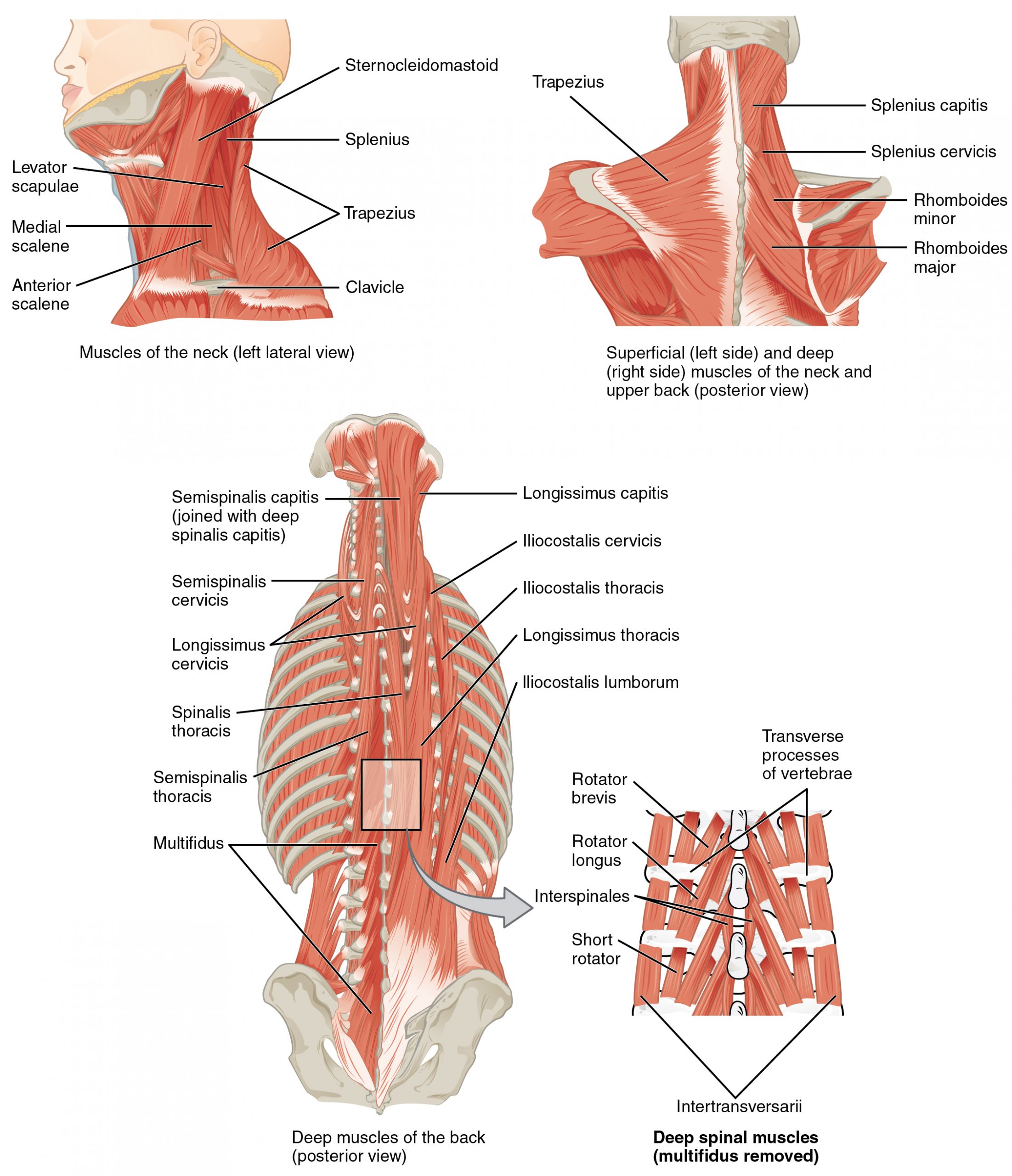{kind=link}
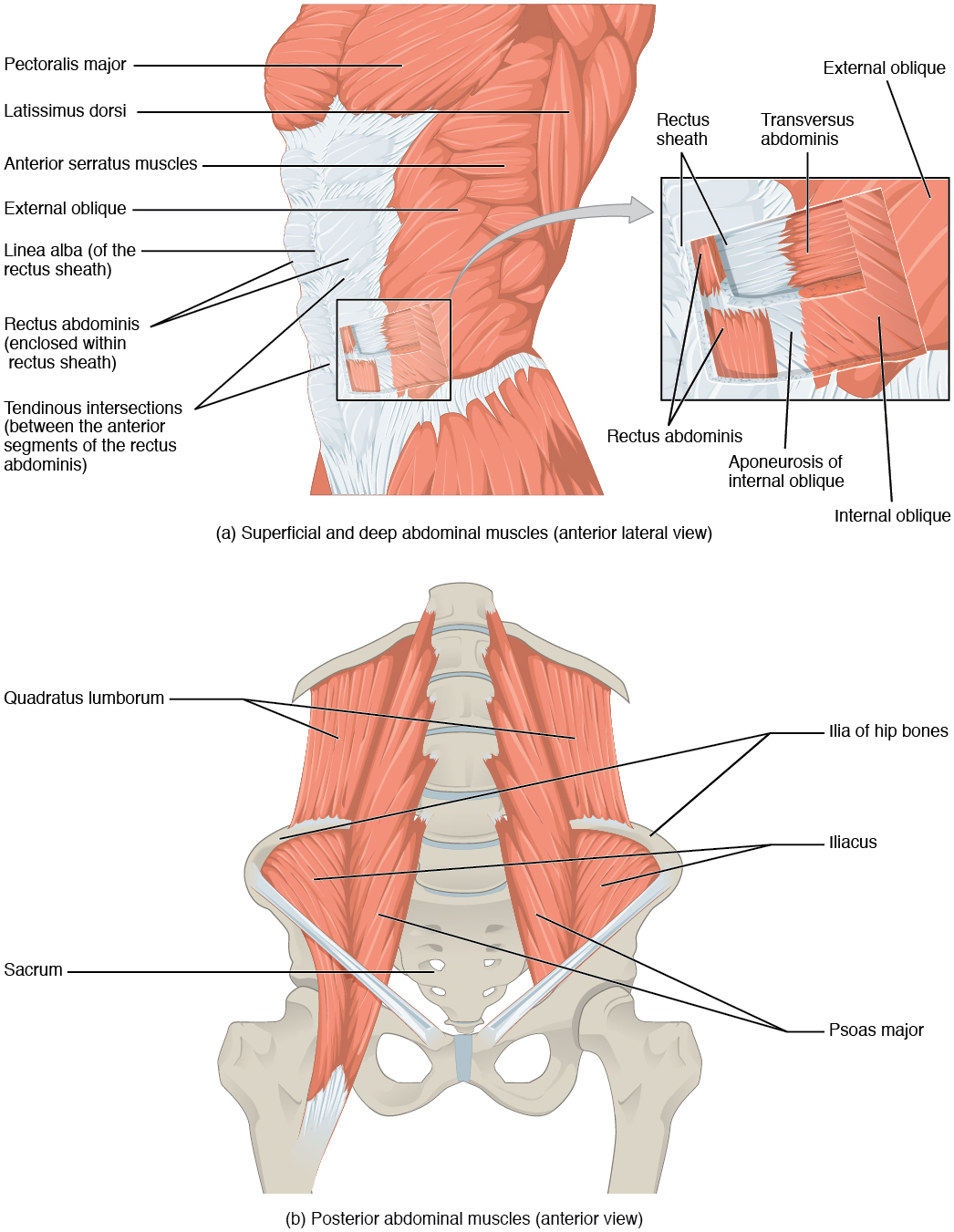{kind=link}
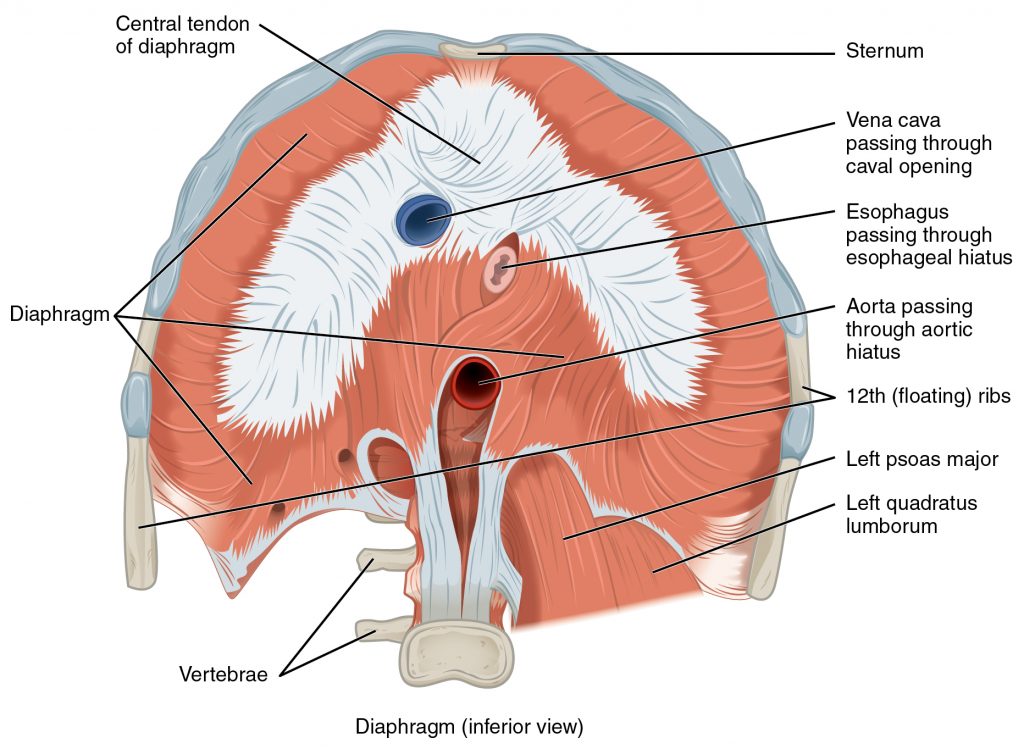{kind=link}
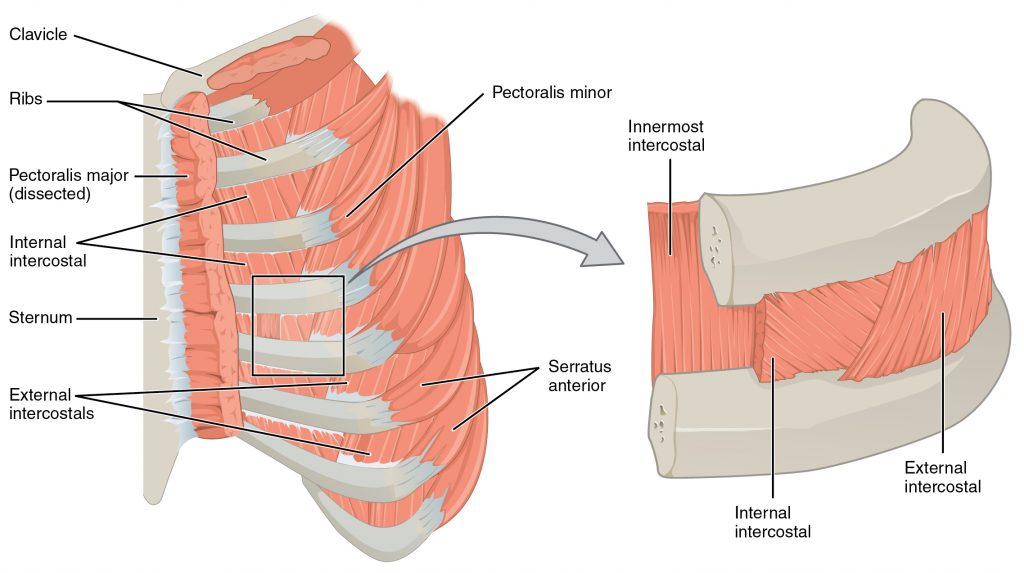{kind=link}
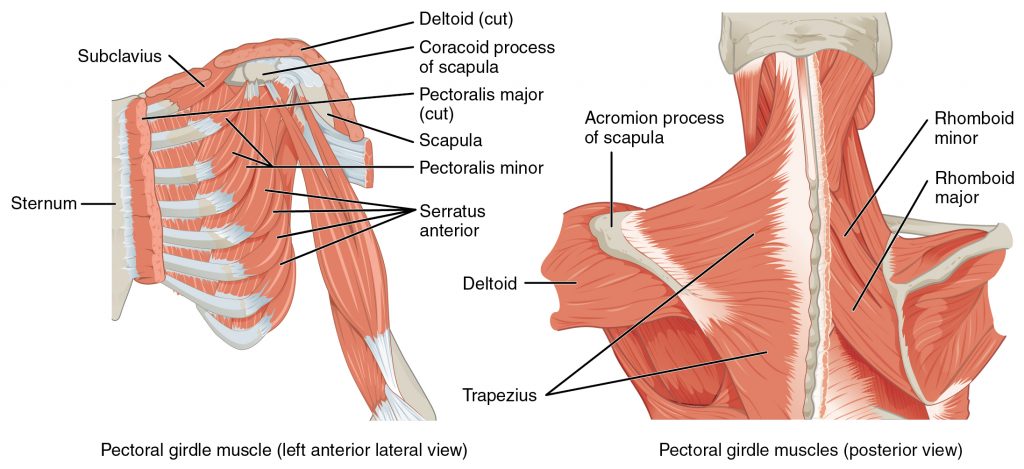{kind=link}
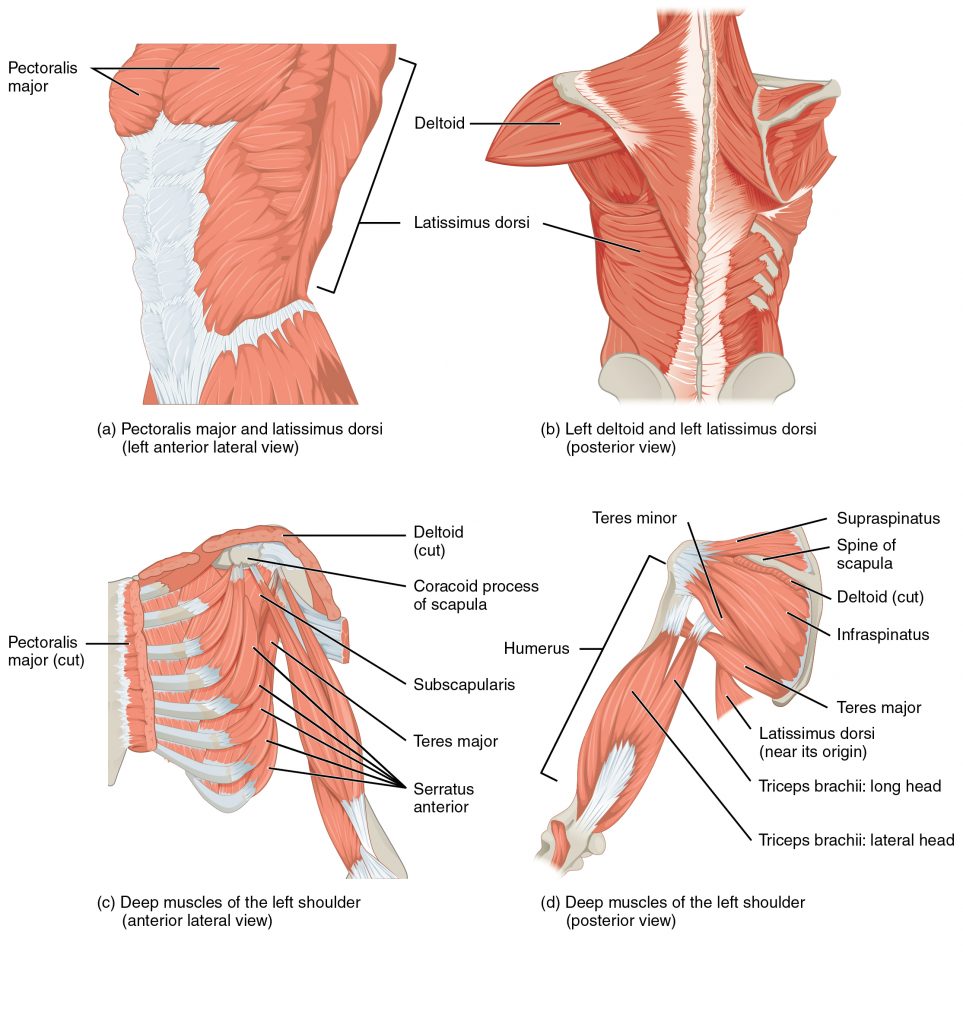{kind=link}
{kind=link}
{kind=link}
{kind=link}
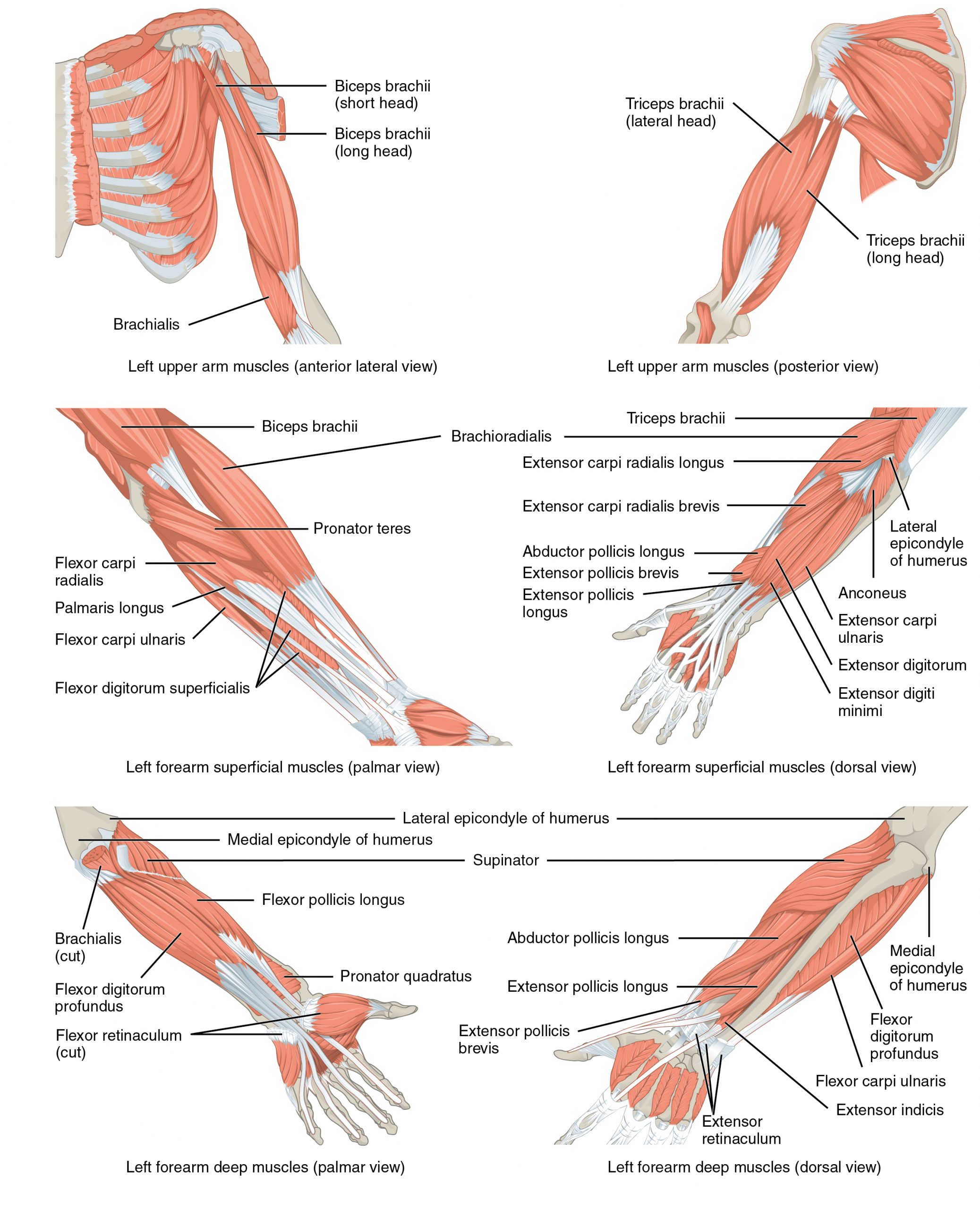{kind=link}
{kind=link}
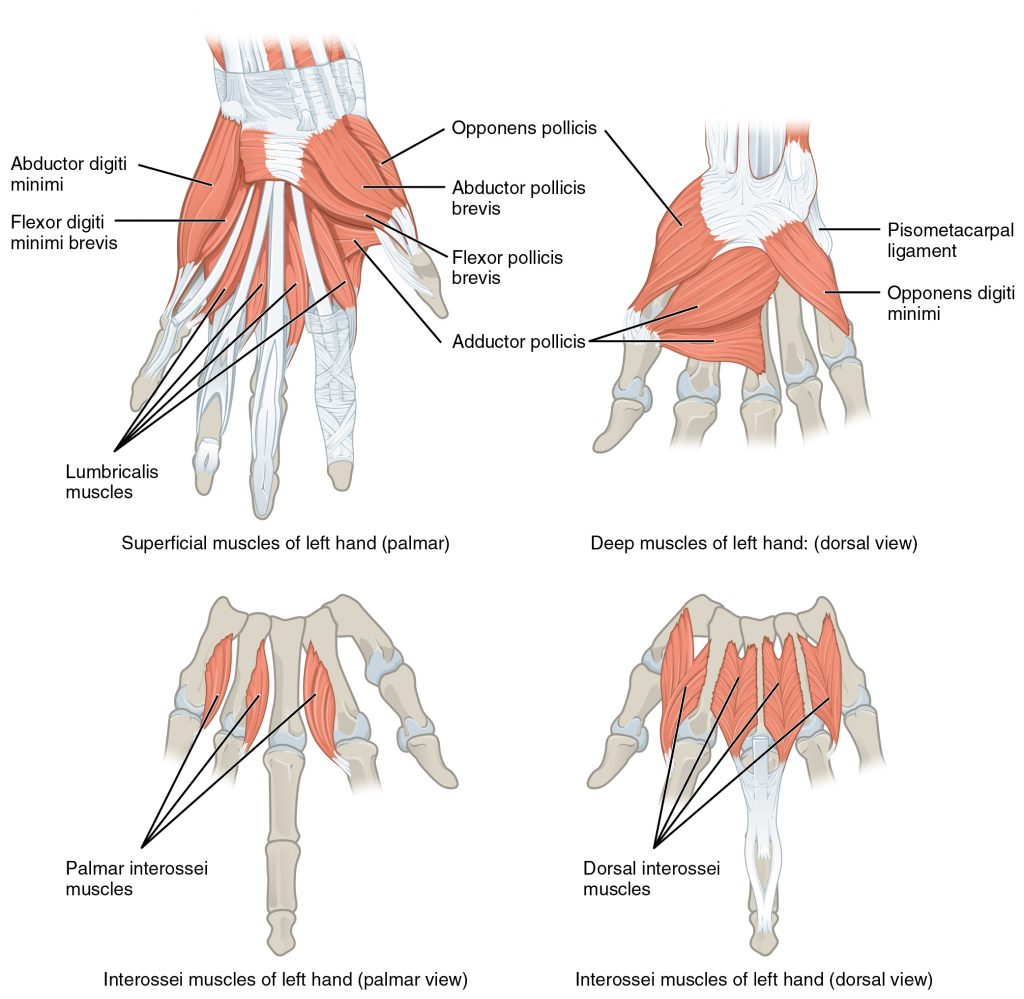{kind=link}
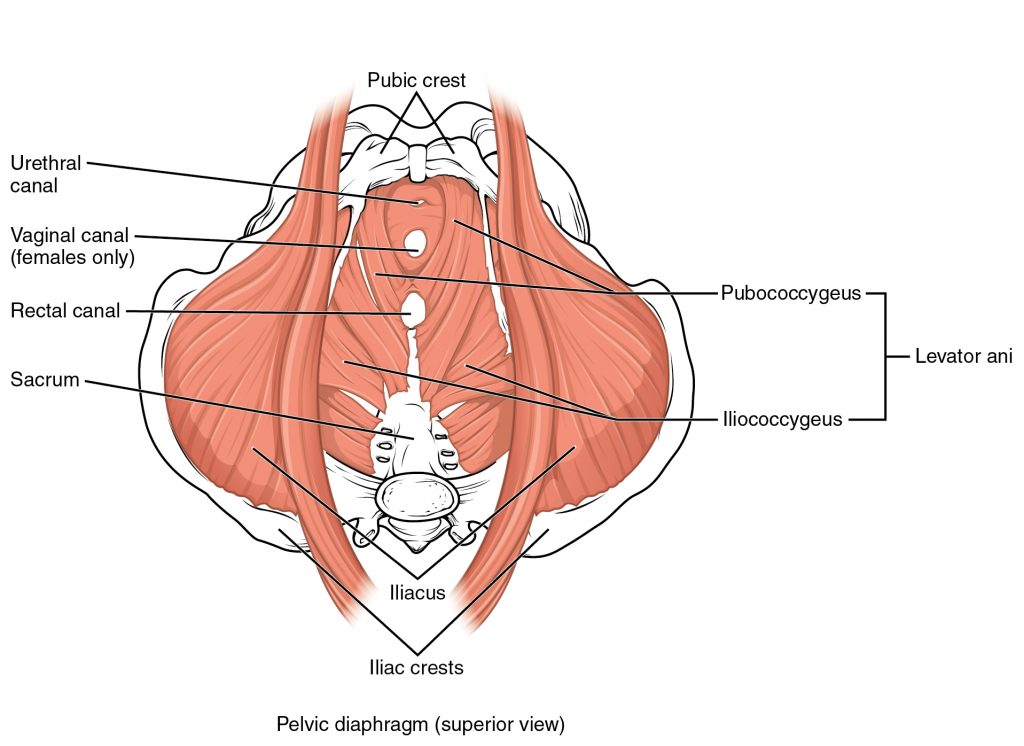{kind=link}
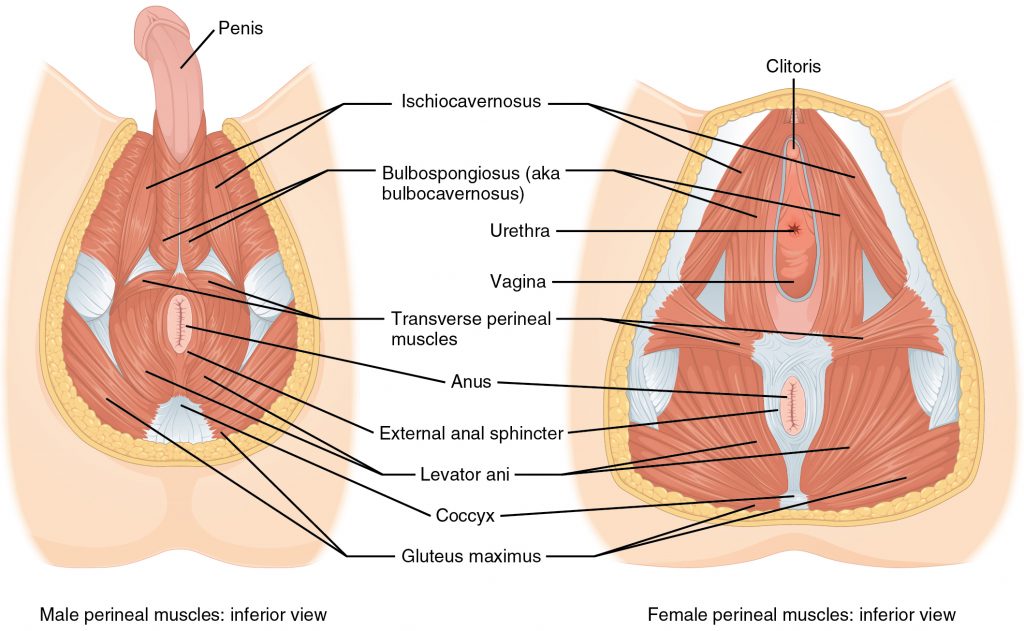{kind=link}
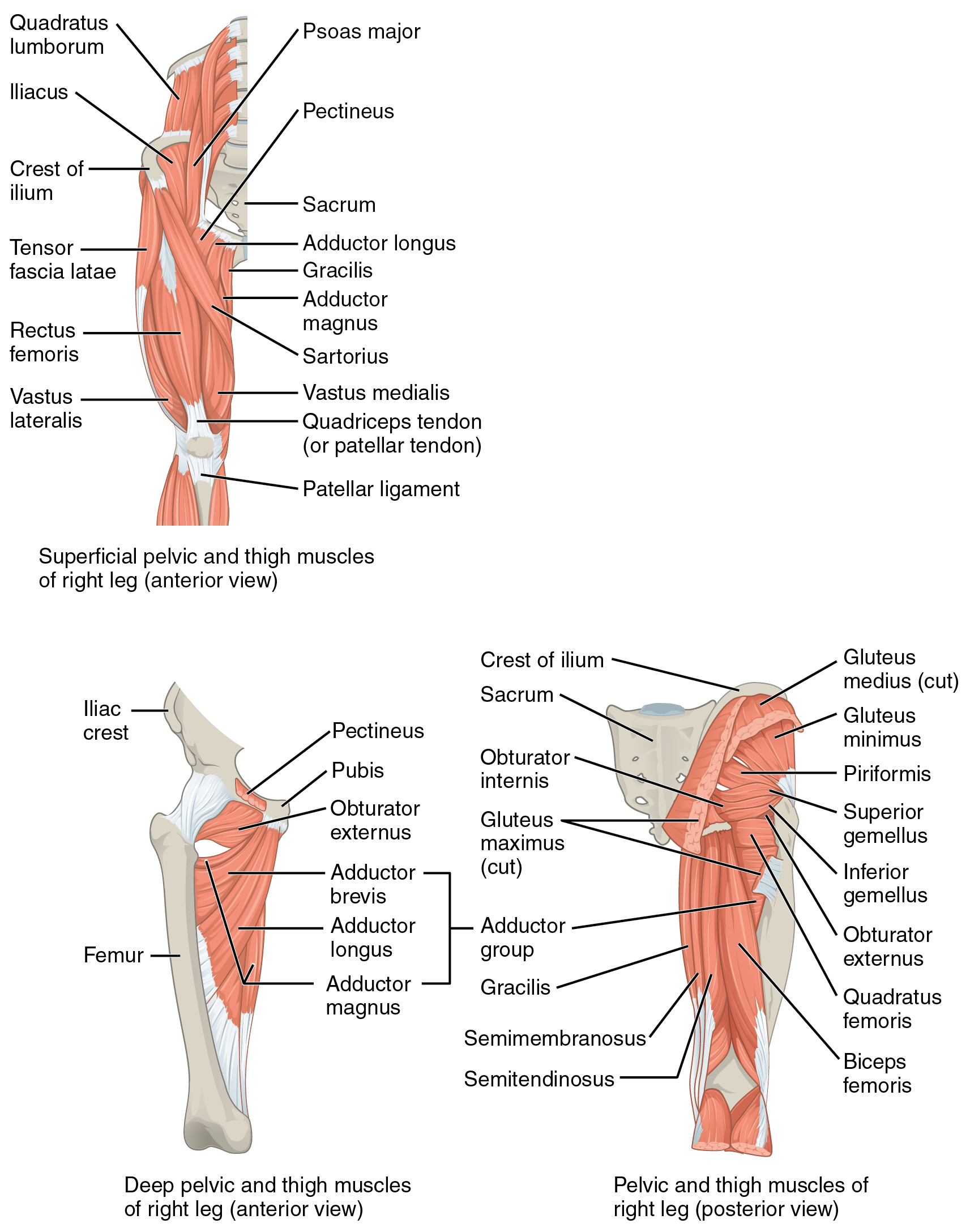{kind=link}
{kind=link}
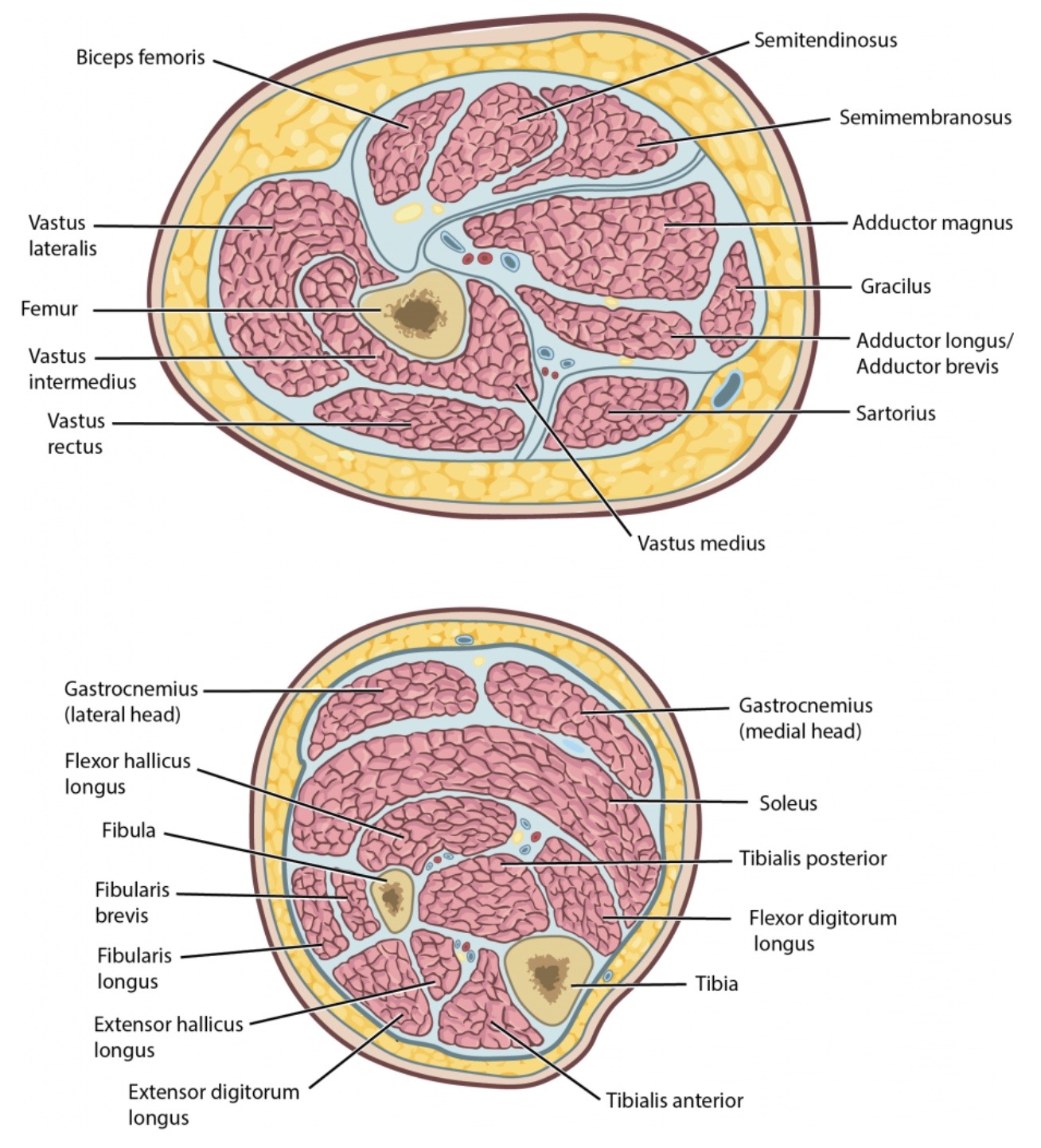{kind=link}
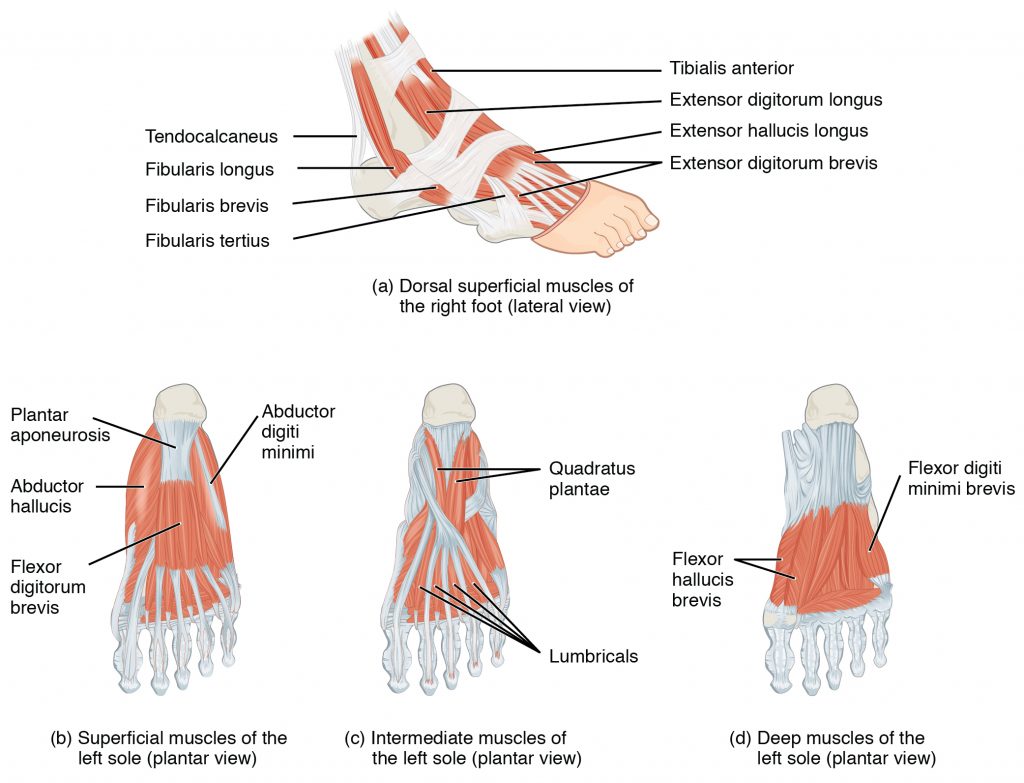{kind=link}