
Chapter 11: Biopsychology of Psychological Disorders
11.6: Post-Traumatic Stress Disorder
Extremely stressful or traumatic events, such as combat, crimes, and natural disasters, place the people who experience them at an increased risk for developing psychological disorders such as post-traumatic stress disorder (PTSD). A diagnosis of PTSD requires that the individual must be exposed to actual or threatened death, serious injury, or sexual violence. This strict diagnostic criterion differs from a common misperception that PTSD could stem from lesser stressors, like for instance, an upsetting but non-violent romantic breakup. Symptoms of PTSD include intrusive and distressing memories of the event, flashbacks (states that can last from a few seconds to several days, during which the individual relives the event and behaves as if the event were occurring at that moment [APA, 2013]), avoidance of stimuli connected to the event, persistently negative emotional states (e.g., fear, anger, guilt, and shame), feelings of detachment from others, irritability, proneness toward outbursts, and an exaggerated startle response (jumpiness). For PTSD to be diagnosed, these symptoms must occur for at least one month.
Roughly 6% of adults in the United States, including 10-12% of women and 5-6% of men, experience PTSD in their lifetime (Goldstein et al., 2016; Olff, 2017), with higher rates among people exposed to mass trauma and people whose jobs involve duty-related trauma exposure (e.g., police officers, firefighters, and emergency medical personnel) (APA, 2013). Nearly 21% of residents of areas affected by Hurricane Katrina suffered from PTSD one year following the hurricane (Kessler et al., 2008), and 12.6% of Manhattan residents were observed as having PTSD 2–3 years after the 9/11 terrorist attacks (DiGrande et al., 2008).
Neural mechanisms underlying post-traumatic stress disorder
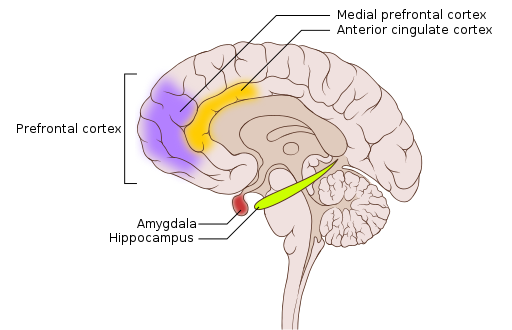
Both the hippocampus and amygdala are involved in emotional processing and have been linked to PTSD (Figure 8). Individuals with PTSD show marked reductions in the volume of several parts of the hippocampus, which may result from decreased levels of neurogenesis and dendritic branching (the generation of new neurons and the generation of new dendrites in existing neurons, respectively) (Wang et al., 2010). However, after effective pharmacological treatment or cognitive-behavioral therapy for PTSD, hippocampus size increases (Bremner & Vermetten, 2004; Levy-Gigi et al., 2013).
Recent work highlights how threat reactivity, the hippocampus, and arousal-related norepinephrine (NE) release may interact to shape PTSD severity. Prior work highlights how threat reactivity (i.e., how someone responds to threat-related stressors) is heightened in PTSD. Research in both animals and humans indicates that norepinephrine, a hormone released in response to stress, is associated with abnormal threat reactivity in PTSD (Naegeli et al., 2018; Southwick et al. 1999). Critically, threat is also known to alter hippocampal functioning, such that reduced hippocampal activity during states of high threat is a reliable neural signature in individuals with PTSD (Eichenbaum, 2001; Hayes et al., 2011). To clarify how threat may disrupt hippocampal functioning, a recent review proposed that threat-related arousal, through heightened NE release, disrupts hippocampal functioning by shifting information processing away from the hippocampus and toward other learning structures involved in emotional memories, such as the amygdala (Clewett & Murty, 2019).
The Advanced Understanding of RecOvery afteR traumA (AURORA) study is a multi-site longitudinal study that assesses individuals who present to US emergency departments within 72 hours of exposure to trauma and tracks their brain and cognitive development for the following year (McClean et al., 2020). This landmark effort will ultimately generate a comprehensive collection of brain, biospecimen, and behavioral measures to better characterize trauma-related disorders, such as PTSD.
To begin exploring the relationship between threat reactivity, hippocampal functioning, arousal-related NE systems, and PTSD symptoms, one AURORA study measured responses to fearful faces in the fMRI scanner and fear-based startle responses to threat cues (a marker of arousal-related NE release) (Tanriverdi et al., 2022). People with more severe PTSD symptoms two weeks after trauma showed weaker hippocampal responses to threat, and hippocampus response was especially reduced in those with a greater fear-based startle. This suggests that excessive physiological arousal from threat may divert information processing away from the hippocampus. These findings emphasize the relationship between threat reactivity, arousal, and hippocampal functioning in understanding how PTSD may or may not emerge after exposure to trauma. Finally, whether or not PTSD emerges is also influenced by genetics, as genes play an important role in the fear and stress circuitry (Banerjee et al., 2017).
Text Attributions
This section contains material adapted from:
Spielman, R. M., Jenkins, W. J., & Lovett, M. D. (2020). 10.4 Emotion. In Psychology 2e. OpenStax. Access for free at https://openstax.org/books/psychology-2e/pages/10-4-emotion License: CC BY 4.0 DEED.
Media Attributions
- Brain PTSD regions © Wikipedia is licensed under a CC BY (Attribution) license
A psychological disorder that develops in some individuals who have experienced a traumatic event. It is characterized by intense, vivid memories of the traumatic event or related events and intense emotional and physical reactions.
(plural form, hippocampi)
A nucleus inside (medial) the temporal lobe implicated in learning and memory.
A neurotransmitter and hormone. Plays an important role in arousal and the “fight-or-flight” response. It is housed primarily in the locus coeruleus.

{kind=link}
{kind=link}