
13 Violence Against People with Disabilities: Implications for Practice
Gabrielle Gault; Alison Wetmur; Sara Plummer; and Patricia A. Findley
Learning Objectives:
- To appraise the relationship between violence and disability
- To document barriers to services for disabled people experiencing violence
- To describe interventions for violence against members of the disability community
Introduction
The abuse of people with disabilities is a historically under-examined and under-researched topic. While the percentage of people with disabilities in the United States (US) is 26% (Centers for Disease Control and Prevention (CDC, n.d.), the physical, sexual, emotional, financial, and disability-specific abuse of people with disabilities is exponentially higher compared to people with no disability (CDC, n.d.). While the specific prevalence of abusive acts remains unclear, the consensus of scholars in this area continually points to anywhere from 50 to 100 percent of people with disabilities being victims of some sort of violence. In fact, some scholars in the field have argued that having a disability will automatically make you a target for some form of abuse (Gilson, DePoy, & Cramer, 2001). Given these high percentages, it would seem logical that more researchers and scholars would focus on interpersonal violence (IPV[1]) of people with disabilities (PWDs[2]). However, this is not the case. This chapter offers a journey through the study of IPV against PWDs by reviewing the current state of the research. The prevalence, forms of abuse, and risks that increase the propensity of abuse will be shared. Current interventions that have been established will be examined using a socioecological perspective. A specific focus on this history of policies created to address IPV in the United States is provided to address the Council on Social Work Education (CSWE) competencies that require a policy-practice approach. The authors conclude this section with how these policies impact PWDs who have been abused.
Given that PWDs have both similar and unique experiences of abuse compared to the non-disabled population, the authors will share information generally about this issue while also choosing to focus on people who are deaf/hard of hearing (d/Deaf[3]). This is in response to our awareness that no one definition and explanation can fully express what occurs to each individual PWD who is abused. A general approach reduces and simplifies this complex and multilayered issue. Suggestions for future research have argued that disability is not a monolith, and new studies must explore the impact of violence on people with specific disabilities and take into consideration the confluence of life experiences based on their unique place in the world (Plummer & Findley, 2012).
This is in response to our awareness that no single definition and explanation can fully express what occurs to each PWD who is abused. A general approach reduces and simplifies this complex and multilayered issue. Suggestions for future research have argued that disability is not a monolith. New studies must explore the impact of violence on people with specific disabilities and consider the confluence of life experiences based on their unique place in the world (Plummer & Findley, 2012).
Intersectionality is a critical concept in understanding the lived experience of PWD, and this chapter strives to discuss intersectional identities wherever possible. In Care Work: Dreaming Disability Justice, Piepzna-Samarasinha (2018) cites a list of principles of disability justice, leading with intersectionality. Another important aspect of disability justice is representation, as demanded by the statement “Nothing about us without us,” a call to establish that PWDs know what is best, are experts in their own lives, and that disability-related issues cannot, and should not be studied without the involvement of PWDs. One of the authors of this chapter is a Deaf woman who is a licensed clinical social worker and thus can adequately share her insights beyond the current research based on her positionality[4]. The authors will share thoughts and suggestions that may be considered in the future to address this issue. Finally, a case study will be presented with various suggestions to address the needs of PWDs seeking support for their abusive situation.
Abuse of PWDs Explored and Defined
Prevalence
The statistics on the prevalence of violence against PWDs suggest that the scale and scope of the issue are significant. Data shows that having a disability not only increases the lifetime risk of experiencing interpersonal violence, but those with disabilities often experience violence for more extended periods of time. In a meta-analysis (Hughes et al., 2012), rates of abuse among PWDs were 1.5 times higher compared to people without disabilities. In their seminal article, Young, Nosek, Howland, Chanpong, and Rintala (1997) examined a community sample to compare rates of abuse between people with and without disabilities and found that disabled people who were abused experienced more forms of abuse for more extended periods compared to people without a disability. More recent studies suggest similar results, indicating that having a disability is associated with a greater risk of violence (Breiding & Armour, 2015), with some indicating a nearly double lifetime risk (Smith, 2007). While the numbers bear witness to a significant problem, it is notable that the field of social work has been slow to explore this issue. This lack of recognition may stem from a reflection of ableism, either intentionally or unintentionally. Ableism is discrimination against PWD in favor of able-bodied people. Ableist norms are easily seen in how social work has mainly viewed disability as a deficiency. As a result, in terms of many social work programs, PWD have been grouped into a singular identity, making it challenging to explore the issue’s complexity (Slayter et al., 2022).
When viewing the experiences of PWD as individuals with intersecting identities, it is possible to unpack the unique risk factors and types of violence that contribute to the alarming statistics. PWDs are at high risk for all forms of abuse and violence in their lifetime, including disability-specific violence, such as withholding medications, over-medicating, and neglecting daily living needs such as toileting and bathing (Plummer & Findley, 2012). More recently, Hahn et al. (2014) found that those who identified as having either a mental health or physical disability were more likely to report having experienced interpersonal violence compared to the general population. Similarly, Haydon et al. (2011) reported that individuals with disabilities had significantly higher rates of forced sexual interactions. Research suggests that more than 80% of women with disabilities experience sexual assault during their lifetimes (Obinna, Krueger, Osterbaan, Sadusky, & DeVore, 2006; Stimpson & Best, 1991). Though men with disabilities experience higher rates of violence than both men and women without disabilities, the majority of research on this topic has focused on the prevalence of abuse of women with disabilities (Mitra & Mouradian, 2014; Plummer & Findley, 2012). While specific numbers may vary, it is believed that 39% of those who identify as female report they experienced rape during their lifetime. People who identify as males with a disability are similarly at higher risk of abuse, with an estimated one-quarter (24%) experiencing some form of sexual violence in their lifetime (CDC, n.d.). Likely a reflection of our cultural assumptions about who can be victimized, there remains a dearth of studies on the abuse of individuals that define themselves as male or nonbinary (Breiding & Armour, 2015). Individuals with multiple identities, such as those who identify as LGBTQ+ or BIPOC, may be further invisible in the data. Without academic exploration, our understanding of prevalence is reliant on self-report or uniform crime reports.
Interpersonal violence, in general, is often underreported. According to the Department of Justice, it is estimated that 2 out of 3 sexual assaults go unreported to police, and only half of domestic violence incidents are reported (2020). PWD may face additional barriers to reporting domestic violence, including lack of education about what constitutes violence, knowledge about individual rights or feeling empowered to exercise them, accessibility of resources, relationship to the perpetrator, or the setting where the violence is occurring. These factors may all compound a survivor’s ability to choose to report.
Some PWDs may rely on the perpetrator for support in daily living, whether in their own homes or a community setting. For those abused in a community setting, institutions may be reluctant to respond. The violence experienced by PWDs may be aided by the systemic silence of the institutions in which abuse occurs. Hospitals, group homes, schools, and medical transportation companies are seldom held accountable for the acts of the individual abuser (Plummer & Findley, 2012). Instead, reports of violence are met with insensitive behavior by service providers and first responders (Swedlund & Nosek, 2000) or are faced with systemic barriers that impede their ability to obtain help (Gilson et al., 2001). Therefore, the issue often gets identified as a micro or singular issue, often framed as the act of a ‘bad apple,’ who is then fired. There is generally no follow-up, policy or procedure review, adjustment in hiring practices, or even a report to the police. This lack of follow-through is due to a need to protect the business or organization from potential lawsuits and a loss of revenue. The fear of news being shared about an incident and its impact on the company’s bottom line prevents the institution’s administration from disclosing violence and abuse. In turn, the individuals who abuse a patient/client/consumer are free to seek out new employment in similar settings, creating a new opportunity for them to harm others. For those experiencing violence in home settings, their experience may be further isolating. The uniqueness of each individual’s experience further validates the need for an intersectional approach that includes the voices of PWDs.
Forms of Abuse
Those who identify as disabled experience all forms of violence and neglect, all of which would be considered abusive. PWDs experience multiple forms of violence and neglect, including physical, emotional, psychological, economic, sexual, and disability-related/specific forms of abuse. Disability-related (disability-specific) abuse can include withholding medications, denying access to mobility or communication devices, neglecting daily living needs, and barring access to medical services (Copel, 2006). This type of abuse focuses on the person’s specific disability and assumed related vulnerabilities. An example would be a partner or family member who intentionally moves furniture and other household items without informing the person who is blind, causing potential accidents and injury. Another situation would be an abuser taking the battery from the scooter of a person who relies on it and placing it at a height the victim cannot reach, thus blocking their ability to utilize mobility aids to leave a dangerous situation. It is essential to consider that an individual with a disability may experience violence due to perceived vulnerability or become disabled due to violence. One example could be a traumatic brain injury caused by ongoing intimate partner violence or mental illness resulting from chronic trauma.
Sobsey pioneered awareness of sexual abuse and assault of PWDs with disabilities in the early 1990s and created the Sexual Abuse and Disability Project (Mansell et al., 1992). Sobsey focused primarily on people with developmental disabilities. Today we continue to see articles that confirm Sobsy’s concerns that PWDs are experiencing sexual abuse and assault at high rates (Tomsa et al., 2021). Today we see that PWDs experience rape, sexual violence not identified as rape, control of reproductive or sexual health, stalking, and psychological aggression at rates higher than those without disabilities (Breiding & Armour, 2015). Sexual assault in all forms can result from intimate partner relationships and professional ones. Some doctors, nurses, care attendants, and transportation drivers have used coercion and threats to engage in intimate relationships (Plummer & Findley, 2012).
Risk Factors
Risk factors for the victimization of PWDs maybe be experienced at the individual, relationship, community, and societal levels. Some factors include having a lack of independence (often defined as dependence) either physically or financially, isolation, a lack of identification of the abuse (especially if it is disability related), learned helplessness (which has been supported by some and deemed victim-blaming by others (Wanjiru, 2021), and the sheer number of people they interact with daily (Hassouneh-Phillips & Curry, 2002; Plummer & Findley, 2012). At the relationship level, PWDs are often asexualized and therefore do not receive education about consent, boundaries, or healthy relationships (Mailhot Amborski et al., 2021). Further, some PWD are not given autonomy to make their own decisions, including about their own bodies, and may internalize this helplessness. At the community level, PWD may face poverty compounded by being on a fixed income or may experience isolation due to a lack of resources or transportation. At organizational levels, there may be a lack of resources, limited experience or training, and implicit bias. At the societal level, bias and attitudinal barriers play a prominent role. Negative attitudes about people with disabilities and other marginalized identities, such as BIPOC and LGBTQ+ folks, dictate how individuals are perceived and treated. Survivors of IPV are often disbelieved; the same is true for survivors with disabilities.
Overarching all these factors and the most influential and damning risk factor, posited by the authors of this chapter, includes the overall devaluation of PWDs in society. As Plummer and Findley (2012) succinctly state, “The scarcity of information about the abuse of women with disabilities suggests a continued reluctance of society to acknowledge that violence toward this population may be occurring” (p.15). The lack of acknowledgment of men’s victimization may be further compounded by cultural assumptions regarding who can be victimized. Generally, attitudes toward the disabled population have been historically negative (Hassouneh-Phillps & Curry, 2002). PWDs have always been marginalized, hidden in locked facilities, dehumanized, and made to feel like a stress and strain on the rest of the population (Cramer et al., 2003). Regardless of disability, PWDs are seen as burdens that must be dealt with rather than integrated into society (Cramer et al., 2003). This, in turn, creates a lack of attention and priority to an endemic that places PWDs at high risk of abuse in all areas of their lives, beginning in childhood.
Ultimately, the cause of IPV rests with the perpetrators of violence. While there are risk factors for victimization that require attention, there are also risk factors for perpetration that demand intervention to ensure that violence against PWD stops. Some individual risk factors for perpetration may include a lack of empathy or adherence to traditional gender roles or hyper-masculinity. At the relationship level, experiencing or witnessing abuse as a child or having an unsupportive family environment could be a risk factor for perpetration. At the community level, poverty, lack of resources, community support for violence, or weak sanctions for perpetrators could contribute. Norms that support violence, including patriarchy and weak policies related to violence and equity, may contribute to perpetration at the societal level. When examining interventions, it is essential to consider responses that address issues at all socio-ecological levels and also seek to prevent harm from occurring in the first place (CDC, n.d).
Interventions
Interventions focused on IPV and PWDs tend to exclude clients’ specific and contextual needs and their unique experiences in the world (Plummer & Findley, 2012). Effective interventions require action at the individual, relationship, community, and societal levels and should target risk factors for victimization and perpetration. Following a public health model, primary, secondary, or tertiary interventions may occur. Primary interventions occur before violence has been perpetrated, secondary interventions focus on preventing escalation, and tertiary interventions are provided after violence has occurred. Within this model, a primary intervention could be educational programs aimed at preventing violence, a secondary intervention could be screening for violence, and a tertiary intervention could provide follow-up services or resources.
Often interventions for PWD focus on the tertiary level and are reactive. This supports the idea that PWDs need to be protected rather than empowered with information promoting a “response-to-risk approach to a broader approach encompassing safety as part of quality of life and human rights.” (Araten-Bergman & Bigby, 2020). These interventions usually focus on skills training for staff working in care settings or behavioral training for PWD on what to do if they experience violence. Secondary interventions such as screening tools for PWD are scarce, limited to physical disability, or center on women’s experiences (Curry et al., 2004; McFarlane et al., 2001). Further, provider training on how to implement screening tools is limited. Existing primary interventions often seek to modify rather than build interventions with input from those with lived experience. For example, programming curricula that seek to prevent sexual, dating, and domestic violence exist; however, programs created for and with the input of PWD are severely limited, as are rigorous evaluations of the modified interventions that do exist (Mikton et al., 2014; Barger et al., 2009).
As noted, the experiences of PWD cannot be grouped into one monolith. Interventions must be developed to meet the individual needs of each survivor based on their experience and available resources or lack thereof. “A comprehensive, trauma-informed response to IPV for women with disabilities must begin by addressing the full constellation of disability-related risk factors and consequences of abuse, at both personal and structural levels” (Ballan & Freyer, 2017, p. 134).
It is relevant to consider that all program interventions are shaped by the implicit bias of the authors, which may limit the scope of content and frequently center women’s experiences. The exclusion of men, LGBTQ+ folks, and BIPOC from intervention development creates an added risk factor for these individuals. For this reason, those with lived experience must be included in the research, development, and evaluation of prescribed interventions. Cross-sector collaboration is also a vital community-level intervention that can propel sustainable change and ensure that victim service providers feel competent to serve PWD and those working in disability-focused agencies feel prepared to empower survivors. While the anti-violence movement and disability justice share tenets of equity and inclusion, they also share a divergent history.
The History of IPV Policy
Overview
Understanding the historical context of how the United States has addressed IPV from a policy and practice standpoint is essential. History offers insight into how a problem becomes a social issue at the forefront of national policy concerns. Public policy has been rooted primarily in attempting to address and respond to ‘violence against women’ and has only begun to address interpersonal violence more broadly within the last decade. Therefore, using the term ‘gender-based violence’ in public policy is intentional—currently, three significant federal policies focus on gender-based violence in the U.S. The following section will outline these policies, including how the legislation impacts survivor-focused programming for PWD locally. Further, there will be a brief discussion of Covid-era legislation and its impact on survivor communities, especially d/Deaf individuals and PWDs. Finally, this section will explore the Americans with Disabilities Act as it applies to survivors of gender-based violence, including opportunities for continued discourse and policy growth.
Federal policy plays a significant role in determining funding allocations and service provisions for survivors of gender-based violence. Federal policy also has the power to shape public discourse, shift perspectives, and generate systems change. To understand the role that public policy plays in the intersection of gender-based violence and disabilities, it is essential to consider how the interpersonal violence field has gotten where we are and to examine how policy can shape where we are going.
Policy Development and Research Trends
Although we now understand that gender-based violence results from intersecting individual, family, community, and societal factors, this understanding was not always widely held. Until the 1970s, in the United States, gender-based violence was viewed as an individual or private issue and was treated as such by the law. Gender-based violence is rooted in patriarchy or the belief that men inherently hold more power than and over women. Patriarchy presumes that there is some innate difference between genders and attaches power to that difference. Within this belief system, men are expected to be strong, aggressive, and dominant and may use violence to maintain that dominance. These same patriarchal views have been codified in law for centuries, from a Roman marriage, where a wife was completely under her husband’s legal control, to marital rape– which was not made illegal in all 50 states until 1993. As of 2023, states’ definitions of marital rape vary to varying extents (Kamp, 2020; Berger, 2006). It has taken decades of awareness-raising, advocacy, and, quite frankly, the death and injury of many individuals to shift gender-based violence into the public sphere, where it is now recognized as human rights violation (United Nations, Office of the High Commissioner for Human Rights, 1993).
Built on the foundation of Civil Rights, Black Liberation, and movements against war in the 1960s, the Women’s Liberation Movement opened a space for survivors of gender-based violence to begin speaking up and working together in grassroots movements for change, except for survivors with disabilities (Evans, 2015). The voices of disabled individuals were often excluded in these spaces prompting the growth of Disability Rights as a parallel movement (Anti-Defamation League, 2018; Price, 2011). There is still an exclusion of PWDs from social movements focused on IPV, as seen during the rise of the #MeToo movement in 2018, prompting the #DisabilityToo movement in response (McNamara, 2018). Notably, women of color were and still are excluded from feminist spaces. Crenshaw (1991) posits that “because of their intersectional identity as both women and of color within discourses that are shaped to respond to one or the other, women of color are marginalized within both. Even the #MeToo movement noted above and birthed by Tarana Burke, a woman of color, did not gain traction until Alyssa Milano, a famous white woman, co-opted the hashtag. In response to the growth of #MeToo, Burke (2017) shared in a Washington Post article that:
What history has shown us time and again is that if marginalized voices — those of people of color, queer people, disabled people, and poor people — aren’t centered in our movements, then they tend to become no more than a footnote. I often say that sexual violence knows no race, class, or gender, but the response to it does (para. 11).
Furthering the point, activist Vilissa Thompson highlighted the exclusion of women of color from the #DisabilityToo movement and responded with #DisabilityTooWhite, which reminded people that disability rights and civil rights are the same (Dunn, n.d.). The intersectionality of oppression is not a new concept, nor is the whitewashing of people of color from mainstream movements. In her book, Black Disability Politics, Schalk (2022) reminds us that although the Blank Panther Party (BPP) “understood disabled people, along with other people of color, people in poverty, women, and gays and lesbians, to be fellow oppressed members of society who had to fight for survival in an oppressive capitalist system”, this narrative is largely invisible in our understanding of the BPP or the disability rights movement (p.30).
During the 1960s, although grassroots activism was gaining national attention, individuals in the community were still being harmed, often behind closed doors. Advocates seeing the need in their communities began opening their homes to create safe spaces for survivors. By the early 1970s, acknowledging that the need was more significant than what individual homes could offer, advocates began to open community-based domestic and sexual violence programs (Fernandes-Alcantara & Billings, 2021). It is essential to consider that this grassroots movement continued to grow in response to community needs; however, there was still no federal legislation or intervention in place to protect survivors or prevent violence from occurring during this time. Additionally, while opened with good intentions, these community-based programs did not consider the unique needs of survivors with disabilities and were often inaccessible (Dubin, 2007). It was not until 1986 that Abused Deaf Women’s Advocacy Services (ADWAS) was founded in Seattle, Washington, to support and empower Deaf and DeafBlind survivors of domestic/sexual violence. ADWAS was the first agency of its kind in the United States. The Department of Justice later funded it in 1998 and 2009 to train other cities in their model (Abused Deaf Women’s Advocacy Services [ADWAS], n.d.).
The elevation of survivors’ voices during this time, as well as a growing national crime rate, prompted the federal government to pay greater attention to violence against women as a public health issue; however, the fight for dedicated funding and legislative change was hard-won. Despite data showing the prevalence of gender-based and family violence, gaining bi-partisan support was challenging through the 1990s. Although during the late 1970s, the Carter administration had secured a meager amount of funding for domestic violence shelters and founded an Office of Domestic Violence in the United States, that funding was later discontinued by the Reagan administration, leaving agencies and families to fend for themselves once again (Weldon, 2022, p.2; NY Times, 1983) With continued public discourse in 1984, the Department of Justice (DOJ) issued a report that examined the scope and impact of domestic violence in the US. This report recommended improvements in law enforcement and community responses to offenses which, in turn, prompted a series of congressional hearings during the late 1980s and early 1990s held to understand better the scope of domestic violence and other forms of violence against women in the United States (Fernandes-Alcantara & Billings, 2021).
While hearings and research continued to explore the scope of the issue, individuals were still being harmed. Critics of the lack of government intervention, like June Zeitlin, former Director of the Office of Domestic Violence under President Carter, seeing that lives were being lost at the expense of politics, noted that “these families need help, not more studies of the problem and election-year rhetoric (NY Times, 1983).” Federal policy cannot advance without bi-partisan support. Looking back at this period, Scholar Van Eck argues that it was a change in rhetoric by advocates from one of patriarchy to that of civil rights and equal protection under the law that eventually pushed the movement forward (2017). For context, in 1984, out of 435 members of Congress, only 24 of those were women (Congress Profiles, n.d.; History of Women in the US Congress, n.d.). Seeking to garner bi-partisan support for legislation that a large percentage of Congress may have felt unaffected by or rhetoric they may have felt attacked by could have stalled support.
The three primary national policies focusing on gender-based violence that exist today are a result of ongoing legal battles, relentless advocacy fueled by the Women’s Liberation Movement, research into the prevalence of the issues, and the bravery of survivors who put a face to the issue by sharing their stories during Congressional hearings. As noted, the voices of disabled people and people of color were silenced during the evolution of the mainstream Women’s Liberation Movement. Conversations and meetings were often inaccessible or invisible in mainstream media (Price, 2011; Schalk, 2022). This systemic exclusion at the very root of the movement meant that disabled voices and Black, Indigenous, and People of Color (BIPOC) were left out of research, policy, and funding allocations. The far-reaching impact of ableism and racism, particularly in policy development and roll-out, is an ongoing concern.
Family Violence Prevention and Services Act
The Family Violence Prevention and Services Act (FVPSA, Title III of P.L. 98-457) was the first federal law to address domestic violence. Initially enacted in 1984, FVPSA has been reauthorized multiple times, most recently through the fiscal year 2015. Although the act has yet to be reauthorized since its expiration, Congress has appropriated funds to ensure the continuity of programs. In October 2021, the House passed H.R. 2119, known as the Family Violence Prevention and Services Improvement Act of 2021, which, if authorized, would amend the existing FVPSA. As of May 2022, H.R. 2119 is still pending Senate action. Reauthorization would allow amendments to the law focused on increasing inclusion and access for individuals with disabilities.
In 1984, when FVPSA was enacted, it included both social service and law enforcement responses to preventing and responding to domestic violence. FVPSA focuses specifically on family, domestic, and dating violence, and it does not broadly address interpersonal violence or gender-based violence. The law authorized grants focused on providing services and shelter to survivors and training and technical assistance to law enforcement personnel nationwide. Over the years, the act has been amended to include support for children exposed to domestic violence and teen dating violence. FVPSA currently authorizes three primary activities: prevention programming, domestic violence services and support, and the national domestic violence hotline, which began in 1996. Training and technical assistance for law enforcement were later removed and brought under the Violence Against Women Act (VAWA) umbrella. The U.S. Department of Health and Human Services (HHS) Family and Youth Services Bureau (FYSB) administers funding for the hotline, domestic violence shelters, and direct services to survivors. The Centers for Disease Control and Prevention (CDC), also within HHS, administers the Domestic Violence Prevention Enhancement and Leadership Through Alliances (DELTA) programming.
When the FVPSA was last enacted in 2010 under the Child Abuse Prevention and Treatment Act reauthorization, apart from ensuring the accessibility of hotline access, it did little to address the needs of disabled people explicitly. While it mentions underserved populations[5], the act did not acknowledge the scope of violence against d/Deaf or disabled individuals or earmark funding to meet their specific service needs. Specifically, the 2010 reauthorization notes that applicants for FVPSA funding must demonstrate a commitment “to the provision of services to underserved populations, including to ethnic, racial, and non-English speaking minorities, in addition to older individuals and individuals with disabilities” and that the funded hotline program “shall provide assistance and referrals to meet the needs of underserved populations and individuals with disabilities” (pp. 47-48). Lastly, it mentions that education and planning should “recognize, in applicable cases, the needs of underserved populations, racial and linguistic populations, and individuals with disabilities” (p. 51). While the act requires a commitment by applicants to provide services for and meet the needs of disabled survivors, it does not offer funding to build agency capacity or support access needs (Family Violence Prevention and Services Act, 2010). This means that although anyone receiving FVPSA funding is committing to serve individuals with disabilities, they may not know how or have staff who feel competent to serve and may not be able to access training. Further, they may be unable to ensure that their facilities, outreach, or services are accessible. As another example, this could mean not being able to develop linguistically or visibly accessible outreach materials or being able to hire a certified interpreter.
Being committed to providing services for disabled people is not the same as being competent or able to provide service. As noted, a primary exception to this is a relationship forged between the National Domestic Violence Hotline and Abused Deaf Women’s Advocacy Services (ADWAS). In 2003, the National Domestic Violence Hotline partnered with ADWAS to roll out the Deaf Hotline. Since 2017, The Deaf Hotline has been available 24/7. Their website “offers safe, confidential advocacy services for Deaf survivors and service providers [and] resources and education about the need for Deaf abuse outreach programs.” (n.d.) This program, however, is not codified in any law but instead supported with discretionary funding.
Contrary to the limitations of the current FVPSA as enacted, bills have been presented in the last few years to amend the act, addressing the erasure of individuals with disabilities from the legislation. One such bill, the Family Violence Prevention and Services Improvement Act of 2021 (H.R. 2119), was passed by the House on October 26, 2021, but was never passed by the Senate. The Senate companion bill S. 1275 also stalled. H.R. 2119 explicitly acknowledged the disproportionate rates of domestic, dating, and family violence among d/Deaf individuals and individuals with disabilities and, as such, would have allowed subgrant funds to be used for “making improvements in the accessibility of physical structures, transportation, communication, or digital services” (p. 29). Subgrants are grants by which funds from one organization are awarded to another agency or sub-recipient to help further the work.
Further, the bill outlined an expectation that funded National Resource Centers and Technical Assistance providers would help increase the “capacity of community-based organizations serving individuals who are Deaf and individuals with disabilities to respond to and prevent, domestic violence, dating violence, and family violence.” That training and advocacy around prevention would consider “community-based programs serving Deaf individuals and individuals with disabilities” (H.R. 2119, 2021, pp. 42, 82). If enacted, H.R. 2119 would have ensured that the barriers and needs of d/Deaf and disabled people might be acknowledged, lending funding, structure, and accountability to the law. Further, it would lead service providers to seek competence in reaching and serving PWDs. The FVPSA has not been reauthorized since 2010, leaving funded programming open to federal budget cuts and limiting expansion efforts like those proposed by H.R. 2119.
Victims of Crime Act (VOCA)
In 1984, the Victims of Crime Act (VOCA, P.L. 98-473) was passed, and through its enactment, the Crime Victims Fund (CVF) was established to provide financial support for state victim compensation and assistance programs. In 1988, the Office for Victims of Crime (OVC) was formally established within the Department of Justice (DOJ) to administer VOCA programs. Unlike other federal streams, VOCA programs are specifically funded through federal criminal fines and fees deposited in the Crime Victims Fund (Sacco, 2021). Within the last several years, CVF deposits have been declining, leading to the July 2021 passage of the VOCA Fix to Sustain the Crime Victims Fund Act of 2021 (P.L. 117-27). Although VOCA applies to victims of any violent crime, it is the largest source of federal funding for domestic and sexual assault services in the country (Buchbinder, 2021).
Each year, Congress establishes a cap on the distribution of VOCA funds. For FY22, $2.6 billion was made available for VOCA-authorized programs (United States Senate, Committee on Appropriations, 2022). This appropriation supported the Children’s Justice Act program, U.S. Attorney General Victim Witness and FBI Victim Witness Specialist staff, and the Federal Victim Witness Notification System. The remainder supported discretionary programs and formula grants. Victim Compensation and Victim Assistance formula grants are distributed to states and territories annually. Victim assistance funds may be used to provide grants to support direct services to victims of crime, including information and referral services, crisis counseling, temporary housing, criminal justice advocacy support, and other assistance needs. Compensation funds may be used to reimburse victims of crime for out-of-pocket expenses such as medical and mental health counseling expenses, lost wages, funeral and burial costs, and other costs authorized at the state level. Discretionary funds have been used for various programs and initiatives over the years. VOCA funds have also been used to authorize programs under the Violence Against Women Act (Sacco, 2021).
Although the Victims of Crime Act does not explicitly mention d/Deaf or disabled survivors, the Office of Victims of Crime (OVC) has shown great dedication to increasing awareness and access for survivors with disabilities. In the late 1990s, OVC funded one of the first national scope initiatives focused exclusively on the issues associated with crime victims with disabilities. Then in January 1998, the National Organization for Victim Assistance (NOVA) used OVC funds to coordinate Working with Crime Victims with Disabilities, a symposium that brought together experts from disability rights, protection and advocacy, crime victim assistance, law, and research. Later that year, OVC published Working with Victims of Crime with Disabilities (NCJ 172838), a bulletin addressing the issues that have created and perpetuated obstacles to safety, services, and justice for disabled survivors, including recommendations on how to improve access (Tyskia, 1998).
OVC has continued to use discretionary funds to support d/Deaf and disabled survivors and improve services by funding initiatives to create fact sheets, training and technical assistance programs, awareness campaigns, videos, and toolkits aimed at increasing capacity for agencies, especially law enforcement, to serve survivors with disabilities. In 2017 the National Resource Center for Reaching Victims was developed with OVC funding and led by the Vera Institute of Justice (www.reachingvictims.org, n.d.). This collaboration is meant to update and expand the field’s resources on crimes against PWDs and seeks to build community capacity by facilitating an online resource library. The library gives the public access to videos and online training, including a toolkit to increase law enforcement’s capacity to work with survivors with disabilities. In the Fall of 2021, OVC recently funded the Vera Institute of Justice to develop a “National Sign Language Interpreter Bank for Victim Services,” which will provide free sign language interpretation services through virtual technology to survivors across the country (Department of Justice, n.d.). Having been recently funded, this program is still in the stages of development ((Vera Institute of Justice [DeafHope Team], 2022)). OVC has also continued to support ongoing awareness-raising about violence against d/Deaf and disabled individuals, particularly during Crime Victims Awareness Week, which takes place each April.
Violence Against Women Act (VAWA)
Initially passed in 1994, the Violence Against Women Act (VAWA, Title IV of P.L. 103-322) is considered landmark legislation as it offers a federal legal intervention into what had been previously considered a private issue. While the Family Violence Protection and Service Act (FVPSA) is focused primarily on service provision, VAWA broadens federal response to gender-based violence by including investigation and prosecution of crimes, providing additional services to victims and those who cause harm, and educating the criminal justice system and other stakeholders about the issue. VAWA covers four primary focus areas: domestic violence, sexual assault, stalking, and dating violence. Provisions for survivors of human trafficking are also covered within the law.
Similar to the Family Violence Prevention and Service Act, the passage of VAWA came from decades of grassroots advocacy, research, and a growing interest in understanding the prevalence of domestic and other types of violence against women. Although the FVPSA allocated funds for shelter and direct services, field research and testimony made it clear that there needed to be a more comprehensive response to violence against women, including harsher penalties for perpetrators. As a matter of context, marital rape was not illegal in all 50 states until 1993, validating the long-held notion that what happens behind closed doors stays behind closed doors (Bergen, 2006; Gover & Moore, 2021) or that women are under the ward of their husbands. Gender-based violence festers in silence and within the patriarchal notion that men and masculine identities hold more power than individuals of other identities. For many, the passage of VAWA meant a greater opportunity to increase safety for survivors, hold offenders accountable, and work toward preventing gender-based violence. The act also authorized the creation of the Office of Violence Against Women (OVW) in 1995 to administer VAWA programs (Sacco & Hanson, 2019).
The Violence Against Women Act requires reauthorization every five years. The act was reauthorized in 2000, 2005, 2013, and most recently in 2022, after it lapsed in 2018. VAWA has primarily been seen as a criminal justice approach to violence, encouraging compliance through legal intervention or punishment. However, this approach does little to address the intersectional needs of survivors, particularly survivors who are black, indigenous, or people of color (BIPOC) who face multiple levels of oppression or risk factors for victimization that may not be addressed by the laws that were mainly created by white men or based on the elevated experiences of white women. From the original drafting of VAWA in 1990 to the present day, the stories of people holding privilege are often highlighted by the media or deemed worthy of public attention. The stories of indigenous women, individuals with disabilities, immigrants, and undocumented individuals, often those most impacted or at risk, go unheard. Policies like VAWA are drafted by privileged people who may have biased perspectives. With each reauthorization of federal legislation like VAWA, there is an opportunity to reconsider whose story is not being heard or who is being left out. The Violence Against Women Act Reauthorization Act of 2022, signed on March 16, 2022, will be in effect from FY2023 through FY2027. Each reauthorization has offered an opportunity to expand access for survivors and increase prevention efforts. This seems especially true for the 2022 reauthorization, which expands tribal authority to prosecute non-native perpetrators[6], increases services and support for underserved communities, brings a greater focus on and penalties for cybercrime, and seeks to improve medical, legal, and forensic systems response for survivors (Violence Against Women Act Reauthorization Act of 2022, 2022).
According to the Office on Violence Against Women’s website, OVW currently administers 4 formula-based and 15 discretionary grant programs, established under VAWA and subsequent legislation (www.justice.gov/ovw, n.d.). Funding is awarded to local, state, and Tribal governments, courts, non-profit organizations, community-based organizations, secondary schools, institutions of higher education, and state and tribal coalitions. Grants are used to develop effective responses to interpersonal violence through activities that include direct services, crisis intervention, transitional housing, legal assistance to victims, court improvement, and training for law enforcement and courts. Rape Prevention and Education (RPE) funding is administered through the Centers for Disease Control and Prevention. One of the 15 discretionary grant programs authorized by VAWA is the Disability Grant Program.
When VAWA was originally enacted in 1994, it did not provide specific funding for survivors with disabilities. It wasn’t until the 2000 reauthorization that the Disability Grant Program was included to fund education and technical assistance to better meet the needs of disabled victims of violence. OVW began making grants under the Disability program in 2002. When VAWA was later reauthorized in 2005, the act expanded coverage for disabled victims by including funding for education, training, and services, as well as grants to cover construction and personnel costs for shelters. During this time, the Disability Grant Program shifted to a focus on sustainable change by funding the development of collaborative relationships between victim service providers and disability organizations and also provided funding for the development of model programs. The Vera Institute for Justice was also brought on as a technical assistance provider to increase success and sustainability during this time. Since 2006, the grant program has remained structurally the same with a focus on collaboration, organizational change, resource sharing, and education. In celebration of the 25th Anniversary of the Americans with Disabilities Act (ADA), the Vera Institute for Justice used OVW funding to launch End Abuse of People with Disabilities, a web-based clearinghouse of resources and information for those working at the intersection of survivor advocacy and disability.
While the grant program itself has been structurally similar since 2006, there were a few changes in the text of the law when VAWA was reauthorized in 2022 aimed at increasing inclusion and access. Specific to section 203, also called Grants for Training and Services to End Violence Against Individuals with Disabilities and Deaf People, the text has been amended to state “individuals with disabilities” without specifying gender (VAWA, 2022, p. 809). Several other sections of the reauthorization have also been amended to be inclusive of all individuals rather than a distinct focus on ‘women.’ Similarly, both the section title and text have been amended to ensure “Deaf people” are included as a distinct group of individuals impacted. Throughout the act, in general, when disabled individuals are referenced, the text has been amended to ‘person-first’ language. Specifically, ‘disabled individuals’ has been stricken in each place it appears and replaced with “individuals with disabilities and Deaf people.” Language has also been amended to ensure that “abuse by caregivers” is included as a covered focus by the grant showing a recognition of the unique experiences of some disabled survivors. Cross-training reach has been amended to include ‘first responders’, and there is a focus on enhancing the capacity of agencies to support individuals with disabilities, reflecting a move toward sustainable systems change. There has also been a substantial increase in funding from $9 million to $15 million over the next 5 years, beginning in FY23. Other notable changes throughout the act include the insertion of ‘underserved populations’ in multiple areas, which by federal definition includes those with disabilities. This VAWA reauthorization, with the inclusion of the “Supporting Access to Nurse Exams Act,” will also fund research seeking to understand barriers to access for survivors, particularly in Tribal, rural, and other underserved communities (VAWA, 2022).
Despite some increased inclusion when it comes to the law, there continues to be a disconnect between the fiscal needs raised by OVW and final federal appropriations. The Federal FY22 budget authorized $575 million in total for VAWA programs which is the highest funding level ever; however, this funding amount is still significantly less than what was requested by OVW or included in the President’s budget. Specific to funding for disabled survivors, there is a large gap between OVW requests and the finalized budget. Most notable is that although OVW continues to request the creation of a dedicated National Deaf Services line, it was not appropriated for in FY22 (National Network to End Domestic Violence, 2022). For FY23, OVW has again requested $4 million for the creation of a Deaf Services Line. In their justification, OVW notes that there are only 21 ‘for Deaf, by Deaf’ victim service programs nationwide and that “deaf survivors frequently seek services from mainstream victim service providers, which often are not well-positioned to meet the needs of these survivors. A national Deaf services line will expand the reach of Deaf-specific victim services by providing these services virtually” (p. 56). A deaf services line was last authorized in 2017 when OVW funded the Vera Institute of Justice’s Center on Victimization and Safety to create a plan for establishing a National Deaf Service Line that will enable Deaf victims of domestic violence, sexual violence, dating violence, and stalking to speak directly with a Deaf advocate or an individual who is fluent in their preferred mode of communication via video phone 24 hours per day, seven days per week (US Department of Justice, 2017).
Executive Order 13985
Unlike the other federal policies noted within this section, Executive Order 13985: Advancing Racial Equity and Support for Underserved Communities Through the Federal Government is not a public law, nor does it have funding directly attached. However, this executive order can increase access and inclusion for disabled individuals who have been historically underserved by addressing barriers to inclusion at the federal level. Specifically, the order seeks to promote:
…the consistent and systematic fair, just, and impartial treatment of all individuals, including individuals who belong to underserved communities that have been denied such treatment, such as Black, Latino, and Indigenous and Native American persons, Asian Americans and Pacific Islanders and other persons of color; members of religious minorities; lesbian, gay, bisexual, transgender, and queer (LGBTQ+) persons; persons with disabilities; persons who live in rural areas; and persons otherwise adversely affected by persistent poverty or inequality( Executive Order 13985, 2021).
Since the release of Executive 13985 in January 2021, federal agencies have begun referencing the order on their grant solicitations and specifically considering equity and access in their priority funding areas. For example, a solicitation put out by the Office for Victims of Crime in April 2022 specifically notes that in support of Executive Order 13985, the funder will:
…give priority consideration to applications that include project(s) that will promote racial equity and the removal of barriers to access and opportunity for communities that have been historically underserved, marginalized, and adversely affected by inequality, when making award decisions (OVC, 2022).
Putting in place an order that seeks explicitly to elevate underserved populations, including those with disabilities, in providing violence against women services appears to be a step toward embracing disability justice as a model for change.
Covid-era Policy
In acknowledgment of the increase in domestic and sexual violence during the pandemic, specific funding was made available through federal legislation to support survivors of gender-based violence. Through the Coronavirus Aid, Relief, and Economic Security Act, 2020 (CARES Act; P.L. 116-136), Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 (P.L. 116-123), and the American Rescue Plan Act of 2021 (P.L. 117–2) funding was made available to increase service access through the virtual provision of services and the reallocation of funds to support survivors seeking direct services due to increased need brought on by the pandemic. Specifically, the CARES Act provided additional FY2020 funding of $2 million for the national domestic violence hotline, including hotline services provided remotely, and $45 million for FVPSA formula grants. The Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020 provided funding to the CDC, which used $1.6 million to support domestic violence prevention grants. The American Rescue Plan Act of 2021 authorized $1 billion in supplemental funding for domestic violence and sexual assault services, including $49.5 million for “organizations that help survivors from historically marginalized communities” (Fernandes-Alcantara, & Billings, 2021; The White House, 2022). Each of these allocations was temporary to help mitigate the increased risk of violence and impact faced by survivors during the pandemic. This funding also allowed expanded service access by increasing the availability of virtual services and support. This virtual support even extended into the courtroom, where survivors could obtain a restraining order through virtual means in many states, while under mandatory stay-at-home orders.
Across-the-board funding for virtual access is a great example of how universal design and access can benefit everyone. Disabled individuals often struggle with transportation and communication-based access, and suddenly due to increased funding for virtual services, survivors were able to connect with a counselor or judge online. To ensure support for those isolating at home, the Department of Justice (DOJ) Office on Violence Against Women (OVW) developed virtual technical assistance and guidance about virtual services and supported courts across the country in providing virtual access for emergency requests, time-sensitive hearings, and victim services (White House, 2021). Some of these funding streams also increased the amount of money being allocated to individuals with disabilities through Medicaid coverage and expanded access to virtual services, transportation resources, and physical modifications to increase access. This is not to say the Covid crisis did not compound the impact on disabled survivors, including increased risk of violence and barriers to help-seeking. However, these policies do highlight how the federal system can adapt and consider creative ways to limit barriers to access all the time, not only during a pandemic. Those with disabilities are not just impacted by disability-targeted programs, they are impacted by all policies.
Americans with Disabilities Act (ADA)
While the intention of Section 504 of the 1973 Rehabilitation Act and the Americans with Disabilities Act (ADA, 1990) are to ensure access and inclusion for individuals with disabilities, both fall short in closing the gaps experienced by disabled survivors of gender-based violence. Often, the barriers to access faced by many survivors go beyond the public understanding of what the ADA covers, such as cognitive, psychological, or intellectual access barriers. Further, programs are not necessarily funded to support the access needs of survivors, or the capacity building required to ensure that those working with Deaf and disabled survivors are prepared to do so.
Although the ADA has changed the field for many disabled survivors, the act has limitations. According to Section 36.105 of the Americans with Disabilities Act, disability “with respect to an individual” is defined as “ (A) a physical or mental impairment that substantially limits one or more major life activities of such individual (B) a record of such an impairment; or (C) being regarded as having such an impairment” (1990). This ambiguity can help some survivors; however, it can also leave agencies and businesses free to decide about access needs based on their biases; these biases mean who decides whose needs fall under the ADA. For example, individuals with certain physical or mental health conditions seeking accommodations through the ADA may find that the ambiguity helps them gain the support they need. However, this same ambiguity means those meant to adhere to the ADA may not have clear guidelines to follow and could therefore decline accommodations for someone whose needs do not fit within their interpretation of the guidelines. This is especially true when individuals with disabilities are not included in decision-making processes.
Federal grant programs also rely on the ADA to set a standard for service provision. The ADA is referenced in most federal solicitations, reminding applicants and recipients that programming must be accessible to individuals with disabilities. This is an example of where bias can impact application. Often agencies consider physical accessibility but neglect to apply accessible design to education, materials, web design, environments, policies, and procedures (Mullen, 2018). This level of critique and application is best achieved by including individuals with disabilities. Often agencies may not even realize how exclusionary their services and policies are. Agencies might collect information about disability status when they provide services; however, if disabled individuals do not know the program exists because their outreach is inaccessible, they are not meeting the requirement of the ADA. This bias in data collection also causes an underreporting of the prevalence and impact of violence on disabled survivors.
One of the limitations of the ADA is that it is a voluntary compliance law, so nothing holds agencies accountable (ADA, 1990). There are no benchmarks or reporting requirements as with other civil rights laws. Suppose someone were to report an agency or business. In that case, agencies often note that the cost of fines for being out of compliance is cheaper than the construction or modification costs of being compliant. To help close this gap and support programs in serving disabled survivors, the Vera Institute for Justice developed tools to help both disability agencies and victim service providers evaluate their commitment to and capacity for serving survivors with disabilities. Agencies can also use this tool online. However, much like the ADA, there is no financial incentive or support for embarking on this process outside of applying for and being awarded a grant through the OVW Disability Program.
Interpersonal Violence and Disability in America: Deafness as a Key Example
According to the National Child Traumatic Stress Network (2006), “severe hearing loss or deafness affects approximately 22 out of every 1,000 people” (p. 4). About two million Americans with hearing loss meet the criteria for profound deafness–the inability to hear anything but the loudest of sounds (National Child Traumatic Stress Network, 2006). Most of these two million Americans comprise the American d/Deaf community.
Though many Americans have hearing loss, the d/Deaf community is mainly unknown to the broader hearing public. A common term to describe d/Deaf people is ‘hearing impaired,’ which focuses on what d/Deaf people cannot do—hear[7]. Doing so establishes hearing as the societal norm and infers that d/Deaf people are abnormal because they cannot hear (National Association of the Deaf, 2019). In contrast, members of the Deaf community focus on what they can do and converse in a visually arresting form of manual communication. Often, d/Deaf people live a life of Deaf Gain[8], enjoying fellowship with other d/Deaf people, and taking pride in their sensory difference (Bauman et al., 2014).
Members of the Deaf community typically ascribe to the social model of disability theory, as well as the cultural model, which posits that Deaf people are a cultural minority (Berger, 2013). These models serve as a stark contrast to the pervasive medical model of disability, which defines a ‘disability’ as a deficiency requiring medical intervention to remedy (Berger, 2013). Proponents of the cultural model of disability posit that a group of individuals with a shared disability, like the Deaf community, are not disabled but rather a cultural minority (Berger, 2013). Furthermore, advocates of the social model of disability state that what we recognize as a disability is a socially constructed state in which the world is the disabling factor versus the impaired body part (Berger, 2013). Often, d/Deaf people straddle the divide between these opposing models; d/Deaf people reside in a world that emphasizes the medical model and devalues our experience. The stark reality of being Deaf in a hearing world increases our vulnerability to traumatic exposure (Anderson, Wolf Craig, & Ziedonis, 2016; Anderson, Wolf Craig, & Ziedonis, 2017a; Anderson, Wolf Craig, & Ziedonis, 2017b; Hall et al., 2017; Hall, 2018).
Customarily, the hearing world considers hearing loss a pathological state that requires amelioration, but the Deaf community views deafness as an entry into the Deaf-World. The world of the Deaf is a world rich in the visual of American Sign Language (ASL) and the fellowship of other Deaf people (Bauman, Murray, & Solomon, 2014). The Deaf community is a small, tightly-knit group, and the shared experience of Deafness is often a refuge within the larger hearing world. Although the sense of belonging enriches members, being deaf predisposes d/Deaf people to traumatic exposure. While this sense of belonging enriches members, d/Deaf people are at a heightened risk for every variety of abuse (Anderson, Wolf Craig, Hall, & Ziedonis, 2016).
Additionally, the unique composition of the d/Deaf community as a linguistic and cultural minority group complicates access to treatment. Mental health professionals fluent in ASL and/or culturally aware of the d/Deaf community are rare, and access to mental health and trauma treatment remains a significant barrier for the Deaf community (Anderson, Wolf Craig, & Ziedonis, 2017a). Though members of the Deaf community experience trauma at a higher prevalence than hearing people, interventions that treat trauma are few.
Trauma and Disabilities
Mental health professionals often overlook the increased incidence of trauma within the Deaf community, perhaps since the Deaf community is largely unnoticed in the broader hearing world. Anderson, Wolf Craig, and Ziedonis (2017a) note, “The Deaf community is one of the most underserved and understudied populations in behavioral healthcare, even though the frequency of behavioral health disorders is believed to be higher in the Deaf community than in the general population” (p. 118). Additionally, due to their status as a linguistic minority, members of the Deaf community may be at even higher risk due to the perceived notion that they cannot tell others what is happening to them. Though there are some specialized programs for members of the Deaf community who are experiencing IPV and amazing mental health clinicians who are d/Deaf themselves and provide assistance in ASL on the frontlines, the need for linguistically and culturally accessible services for d/Deaf people greatly outstrips availability.
Recent studies reveal that d/Deaf people are twice as likely to experience trauma as hearing people (Johnson et al., 2018; Schenkel et al., 2014). These types of trauma include physical abuse, unexpected death of family and friends, and natural disasters (Anderson et al., 2016a). ‘Rhonda’ a survivor who shared her story as part of a series produced by the organization, DeafHope, illustrates the weight and experience of compound trauma by sharing:
I want to share my experience with different kinds of abuse. When I see other people experience abuse and share it, it touches my heart. I felt afraid to share because I was scared of gossip and my reputation, and I am a very private person. I stayed silent and wouldn’t share my story for many years. I experience different abuse, and now there is a suitcase full of experiences of abuse I have carried with me for many years. It gets heavier and heavier, and now I can’t carry it anymore.
Many traumas may stem from the fact that d/Deaf people often miss out on incidental learning opportunities, such as hearing that there is impending dangerous weather from a radio announcement or overhearing family members discuss illness and death among loved ones. This lack of access can complicate or trigger a traumatic experience. Johnson et al. (2018) report that d/Deaf individuals are more likely to develop Post-traumatic Stress Disorder (PTSD) than hearing people due to these complex traumas.
Additionally, d/Deaf people may experience developmental trauma triggered by the phenomenological experience of being raised in a hearing-dominant world (Anderson et al., 2016a). Anderson, Wolf Craig, Hall, and Ziedonis (2016a) identify a lack of early language development as a significant factor that increases the vulnerability of d/Deaf people to experience trauma. Other factors include family conflict over education and schools, a preference to have children speak orally rather than use ASL, poor or insecure attachment to parents, and social isolation (Anderson et al., 2016a, p. 353). These stressors predispose a d/Deaf person to a lifeworld filled with trauma and heartache.
Language Deprivation: A Uniquely d/Deaf Trauma
Recent studies show that up to 70% of all d/Deaf people show signs of language deprivation (Hall et al., 2017). Language deprivation occurs when young children do not have access to language (Hall et al., 2017; Hall, 2018). Despite universal neonatal hearing screening, many d/Deaf children are not diagnosed with hearing loss until they are toddlers (Hall et al., 2017). As a result, these children struggle with communication since spoken language and lipreading are difficult without an existing linguistic foundation. To compound these difficulties, only about 40% of spoken English is visible on the lips in ideal conditions with a skilled lip reader (CDC, 2020). Therefore, hearing-abled families’ preference that their d/Deaf family members communicate using spoken language results in an environment where communication is not accessible to their d/Deaf family members.
Recent research indicates that the time window for optimal language acquisition is during the first year of life (Friedmann & Rusou, 2015). If d/Deaf children do not have access to a fully accessible language during that time, they miss crucial opportunities to develop a solid primary language foundation; if people do not have fluency in a language from childhood, problems compound into poor academic performance, frustration with communication that can lead to behavioral problems, interpersonal and inter-relational difficulties, and overall deficits in everyday functioning. Language deprivation also impacts d/Deaf people’s understanding of English, which makes the standard intervention of writing back and forth challenging at times and further complicates their ability to effectively answer written screening questions and tools (Hall et. al, 2019).
Researchers identify prelingual[9] deafness and a lack of exposure to ASL during early childhood as often robbing the d/Deaf of a linguistic foundation (Glickman, 2009; Glickman & Gulati, 2003; Freeman, 2003; Hall, et al., 2017; Hall, 2017). Glickman (2009) states, “Some deaf children may be nearly the only examples of human beings . . . who grow up without native language skills” (p. 375). Lack of developmentally appropriate language acquisition means that some d/Deaf people have minimal language skills at best. Freeman (2003) reports that most of her deaf clients grew up prelingually deaf and lacked ASL exposure during childhood. Freeman (2003) states, “Growing up in this linguistically impoverished environment, these deaf children grow up with emotional, social, educational and psychological delays” (p. 36). Additionally, Freeman (2003) notes, “for the deaf or hearing-impaired client whose trauma may have occurred prior to full linguistic acquisition, the trauma remains unconscious and nonverbal” (p. 36). As a result, people with low language fluency struggle to think abstractly (Glickman & Gulati, 2003), which results in extreme difficulties in accessing health treatment because mental health concepts are largely abstract (Hall et. al, 2017).
Because d/Deaf people with language deprivation have varying grasps of formalized language, additional support is often needed to access services (Anderson et al, 2016; Glickman, 2009; Glickman & Gulati, 2003; Hall, 2017). When utilized, Deaf interpreters for the Deaf serve as communication brokers between the hearing ASL interpreter and their d/Deaf client since a simple English-to-ASL translation will leave someone with language deprivation unable to understand fully what is being said (RID, 2022). However, many hearing providers are unaware of the importance of an additional interpreter to interpret the ASL into visual-gestural communication so a d/Deaf client with language deprivation can fully understand.
Additional complications include a lack of culturally and linguistically trained clinicians to help d/Deaf victims of IPV heal. Anderson, Wolf Craig, and Ziedonis (2017a) note, “The Deaf community is one of the most underserved and understudied populations in behavioral healthcare, even though the frequency of behavioral health disorders is believed to be higher in the Deaf community than in the general population” (p. 118). Most social workers are hearing-abled and may be unaware of the importance of ASL and Deaf Culture to members of the Deaf community. Though the Americans with Disabilities Act of 1990 mandates that healthcare organizations provide ASL interpreters for people with hearing disabilities, many doctor’s offices are unaware of this mandate or reluctant to pay out-of-pocket for interpreters (Boness, 2016). A survivor of domestic violence through the DeafHope Survivor Stories series expressed the feeling of isolation created by the lack of linguistic access, saying:
During my time in the shelter, I was always alone. The televisions were not closed captioned. The interpreters were not provided. There were no communications and no television access. Also, no TTYs. No interpreters during support groups. None. I just sat there alone, feeling left out with information going over my head. I gained nothing from it.
This same survivor went on to express the importance of the availability of culturally specific services when saying:
We need a place of our own, not a hearing shelter, for the Deaf women survivors. We need it. It is also for our hearing children. With this shelter, I would still have my children with me. But right now, we don’t have one…I want for Deaf women to wake up and realize that they don’t need domestic violence, nor deserve it. The children do not deserve it either. It is hard for them to see their mothers go through domestic violence. They want violence-free and healthy homes where they can grow up together with their Deaf mothers.
In his chapter, The Isolation of Being Deaf in Prison, published in Disability Visibility edited by Alice Wong, Jeremy Wood shares his experience with language deprivation and isolation in prison:
While I was in prison they had no American Sign Language (ASL) interpreters. None of the staff knew sign language, not the doctors, the nurses, the mental health department, the administration, the chaplain, or the mailroom workers. Nobody. In the barbershop, in the chow hall, I couldn’t communicate with other inmates. When I was assaulted, I couldn’t use the phone to call the hotline set up by the Prison Rape Elimination Act (a federal law meant to prevent sexual assault in prison) to report what happened. And when they finally sent an interviewer, there was no interpreter. Pretty much everywhere I went, there was no access to ASL. Really, it was deprivation.
Intimate Partner Violence in the Deaf Community
Intimate Partner Violence[10] is endemic in the Deaf community, as it is with others who identify as disabled (Mailhot Amborski et al., 2021). Due to the Deaf community’s status as a minority culture, there are not many studies about intimate partner violence in the Deaf community, but the ones that exist tell a consistently negative tale. A national sample found lifetime prevalence rates of 27.1% for emotional abuse, 22.2% for physical abuse, and 16.9% for sexual abuse for d/Deaf women (Pollard et al., 2014).
Due to language barriers, abusers have additional tools at their disposal. They may deny their victims access to communication with others by taking away or limiting access to cell phones, tablets, computers, and Videophones for texting, email, and video chatting. Since signed languages are minority languages, and most d/Deaf people show signs of language deprivation, an abuser can control a person’s access to communication. A hearing-abled abuser may use their partner’s status as a d/Deaf person to denigrate and marginalize them (Anderson et al., 2017a; Anderson et al, 2017b). In public interactions, a hearing abuser often serves as a communication intermediary between their d/Deaf partner and the hearing world; when an abuser is a conduit through which a d/Deaf person can communicate with a hearing person, the abuser can manipulate what is being said to disempower the abused.
As part of a survivor story series produced by DeafHope, a survivor of domestic violence shared:
I went through “Nine Lives”. I had many close calls with death during my domestic violence experience. However, I am lucky to be alive today. I am a survivor from trying to stay alive. I have tried calling the police several times. My husband blocked me from the phone. He took away the phone. Many times he prevented me from calling because he wanted to keep it a secret. One day the neighbor heard us and called the police. The police came but my husband (hearing) talked to them. They didn’t talk to me much. The police thought that everything was okay and left. They did nothing to help. As soon as the police left, my husband started to beat me up again. This time the neighbors did not want to call the police again.
Additional complicating factors include language deprivation, which limits the abused and the abusers’ ability to express what they have experienced, as well as to explain what is bothering them. Professionals who work with people who have experienced trauma understand that trauma is cyclical, and abusers are often abused themselves (van der Kolk, 2015). Without the ability to express and process previous trauma, d/Deaf people struggle with accessing appropriate treatment and behavioral change (Anderson et al., 2017a; Glickman, 2009).
Language deprivation affects more than someone’s ability to express themselves. If a d/Deaf person does not have a strong language foundation, they may not know that it is inappropriate to hit others or force themselves on others sexually. It is important that those working with d/Deaf clients be aware of possible language deficits and the lack of general knowledge that many d/Deaf people face (Hall, 2017).
Another important consideration is a client’s membership in the capital D-Deaf community. As mentioned before, the Deaf community is small, insular, and tightly knit. Members of the Deaf community tend to be more collectivist in their perception of the world, valuing their membership in the group over their individuality (Bauman et al, 2014). While the Deaf community is often a source of support and fellowship for Deaf people, intimate partner violence can complicate Deaf community membership, especially if both the abuser and the abused are members of the Deaf community. Friends may be compelled to take sides, and due to the collective nature of the community, gossip will abound. Therefore, it may be easier for a victim of IPV to stay quiet about the violence than risk being “outed” by the whole community and potentially losing friends and supporters.
Macro-Policy and Practice Implications for Working with PWDs Who Experience Abuse
Application of Theoretical Perspectives
Types of Disability and Violence
A disability can have a physical, intellectual, sensory, cognitive, emotional, and/or psychiatric basis, and their impairments can be singular or occur in combination, including learning disabilities. We have chosen to use d/Deaf as an example of disability, yet we want to emphasize that disability is complicated and multidimensional (Altman, 2011) and individual. d/Deaf as an example of a disability is illuminating, as it highlights the fact that some disabilities are not visible. Kattari et al. (2018) note that those with invisible disabilities “are still exposed to forms of rejection, ableism, and discrimination; in fact, they may even have more trouble accessing support services than their visibly disabled counterparts due to being expected to prove their disability” (478). For example, those with learning disabilities are more likely to experience hate crimes, harassment, bullying, and name-calling than those with other disabilities (Wiseman & Watson, 2021). Also, those with sensory disabilities are at greater risk for sexual victimization (Amborksi, Bussieres, Vaillancort-Morel, & Joyal, 2021). Moreover, we see those with disabilities, particularly those who fall victim to violence, being part of a disability justice movement focusing empowerment on the individual and the collective rights of all those with disabilities and other marginalized communities.
Abuse and Myths for Those with Disabilities
Pertinent to social work practice is awareness and understanding that society still holds some misunderstandings and myths about how IPV happens for PWDs. PWDs experience multiple forms of abuse, including physical, emotional, psychological, financial, sexual, and disability-related. The approach of the worker with PWDs should include the examination of the workers’ understanding and feelings regarding disability, including ableism and able-bodied privilege, then address their perspectives that do not support a strengths-based practice (Plummer & Findley, 2012). This examination should also look externally at the social forces that allowed the violence to occur, including oppression and other forms of structural inequalities (i.e., poverty) that allow for higher tolerance of maltreatment of PWDs (Hollomotz, 2012).
Critical Cultural Competence
For social workers who work with PWDs, it has become increasingly salient to work with a framework that brings not only recognition of the disability the individual has but, more so, all that comprises the individual. Regardless of disability, this chapter has emphasized that these individuals must be treated with inclusion and respect and be recognized as members of the greater community. This is paramount as violence itself is complex and intersectional. Working with individuals requires understanding the complete biopsychosocial foundation of the individual as well as what having a disability means for that specific individual.
Working in a frame of critical cultural competence requires that social workers develop critical cultural competency by understanding themselves, their clients, and their clients within their communities. Workers need to develop an understanding and awareness of the intersectionalities that their clients bring (NASW, 2015). For example, social workers need to see a client as a parent, a student, a person of color, and an individual with a disability. As social workers, we need to reflect on all that individual brings and how it shapes the client’s social identity while at the same time having an awareness of our attitudes and beliefs about all of those intersecting identities.
Critical cultural competence is an ongoing practice rather than a box to check. This means that social workers are expected to participate in continuing education, training, and consultation that helps them to identify their own biases and minimize the imposition of those assumptions on the individuals they serve. It is also essential to ensure that those with lived experience inform practice. Research and policies, whether agency or federal, practice interventions need to include the perspective of those who will be most impacted.
Self-Determination
Supporting this stance allows one to make choices for themselves and is an integral part of strengths-based social work. This concept has even more relevance when we are working with PWD. We want to support and empower PWDs across the life course. In particular, related to IPV, social workers need to consider our thoughts and beliefs to ensure we are working with PWDs as partners, and we are not disrespecting or infantilizing these individuals. For example, empowering clients to make decisions or choose resources for themselves helps them gain a sense of self-determination.
Nothing About Us Without Us
This phrase provides a solid underpinning that policy about PWDs should only be decided with the full and active participation of PWDs. The consideration of who is involved should include an intersectional and inclusive perspective. Furthermore, social workers must remember that not all with disabilities are similar. Pushing this conversation further, some disability justice advocates have recently modified this call to action to be “Nothing without us!” reflecting the notion that PWDs need to be included everywhere, not only the places someone has deemed to be about disabilities (National Democratic Institute, 2022).
Limitations of Federal Policy: Implications for Practice
There have been strides in the last 30 years to ensure that PWDs are remembered within federal policy administration. However, there is still much more to do; those who are d/Deaf need to be considered and included in advocacy and policy development at the very foundation. Federal policies need a more robust benchmark than a reliance on the ADA for compliance measures as well as programming and services based on non-discretionary funding.
Promote IPV Inclusion in Policy
Federal appropriations for gender-based violence intervention and prevention services are based on a conglomeration of legislation. Community-based agencies rely heavily on federal funding for service provision, which can change frequently based on organizational priorities. Funding priority areas may also change year to year and limit the types of services covered by specific funding streams. The needs of survivors, especially those with disabilities, do not go away because funding does. Further, disabled survivors and their needs should be codified within the law rather than having the ADA, or an Executive Order applied as an overlay to encourage inclusion. Promoting inclusion without financial or other resources means that sustainability will remain impossible.
Primary Prevention is Needed
While there is ample research on the prevalence of violence in underserved communities, there is a dearth of research and money looking at primary violence prevention in the disabled community. Although VAWA and FVPSA money supports primary prevention, there seems to be an expectation that agencies will either modify prevention strategies to meet the needs of individuals with disabilities or focus their education on risk reduction. Things you can do to lessen your risk of becoming a victim.[/footnote], which can prompt victim-blaming and does not stop the perpetration of violence before it happens. Even the OVW Disability Grant does not fund primary prevention programming since that is covered under Rape Prevention and Education grants distributed through the Centers for Disease Control and Prevention (CDC) (CDC.gov, 2022). This is another example of how excluding individuals with disabilities can impact programmatic priorities and outcomes. While the CDC has developed toolkits for communities to address domestic and sexual violence prevention, it neither mentions the unique needs of PWDs nor shares primary prevention strategies that have been vetted for use with disabled populations.
Include PWDs in Research, Evaluation of Programming, and Policy Efforts on IPV
Federal policy is based on research, data collection, program evaluation, and feedback from constituents. When you exclude PWDs at the very root of research and data collection, the policies seeking to reach these individuals will fall short. Further, if the expectation is to stop the perpetration of violence against PWD, then federal policy and funding allocations need to meet that expectation. Policymakers must ensure that communication channels are open for individuals with disabilities to share their concerns and feedback. Programs and agencies need benchmarks to follow and should be evaluated based on their ability to reach survivors with disabilities.
The abuse of people with disabilities is a historically under-examined and under-researched topic. However, there is an awareness that the overall rates of abuse against PWDs are higher than those without disabilities. Moreover, the debate over what constitutes abuse is rooted in the systemic silence of the provider agencies and organizations in which the abuse occurs. Attempts to intervene for those with disabilities who have been abused or assaulted have been reactive rather than preventative and culturally aware. While there has been progress in policies related to PWDs and IPV, work is left to be done to advance the rights and protections of PWDs under the law and in practice. This knowledge should serve as a call to action for social workers and clinicians who need to develop the critical cultural competence necessary to work with individuals with PWDs in this area and to promote policy change.
Case Study
Now it is time for you to take all of this knowledge and apply it to a fictionalized situation. Here are the details of the hypothetical case, based on experiences from the authors’ decades of work in the d/Deaf community.
Scenario: Imagine you are a hearing social worker at a local domestic and sexual violence program serving individuals who have experienced IPV. The program provides crisis intervention services and short-term counseling for all community members but does not explicitly offer specialized services for the d/Deaf. As a result, your knowledge of the d/Deaf is relatively sparse.
Your supervisor tells you there is a new referral for you and mentions that the woman is Deaf. Your supervisor hands you the information packet, which is all of the information you have going into your upcoming meeting with “Maria.”
Maria is a bisexual Latinx woman in her early 30s who lost her hearing due to illness when she was about two years old. Maria communicates in American Sign Language (ASL), but significant general knowledge and language gaps complicate comprehension. Maria reports significant trauma, from sexual molestation at the hands of her brother, sexual abuse while at the residential school for the Deaf, and severe emotional and sexual abuse in her last romantic relationship, which led to the current sexual assault referral.
Like most d/Deaf adults, Maria is the only d/Deaf member in her family. No one else in her family uses ASL to communicate, and Maria says she does not feel a deep connection to her family because she cannot communicate with them. Maria has created her own support system of people in the Deaf community. One of Maria’s support system members is “Kevin,” with whom she has had a sporadic and sometimes abusive relationship. Kevin is a fixture in the local d/Deaf community, and Maria is worried that talking about her problems with Kevin will cause her to be ostracized.
Like many PWDs, Maria lives at or near the poverty line. She relies on Social Security Disability Insurance for her primary source of income, does not have a car or reliable transportation, and relies on numerous government and local agencies for day-to-day support. After an emergency room visit where she stated that she felt unsafe in her romantic relationship, a referral was made to your domestic and sexual violence program for Maria to get counseling and support. Although your agency’s brochure mentions that you provide domestic violence services to all community members regardless of disability status, Maria has never heard of your organization before. Maria lined up medical transportation, but her ride arrived 30 minutes late, which made Maria 45 minutes late for her scheduled appointment.
Unbeknownst to you, upon arrival, Maria realizes that she must push a button and communicate with someone via speakerphone to gain access to the building. Maria enlists the help of a hearing passerby to gain access to the facility. Once inside, Maria is confused about where she must go as there are no signs. Maria starts to wonder if coming here to discuss her recent sexual assault is worth it. She’s also 45 minutes late, and doctors usually get mad at her if she is late to appointments.
Luckily, she spots a woman all in black sitting in the hallway, and taking a chance, she approaches her and realizes that the woman is there to provide ASL interpretation for her. Maria and the woman greet each other, and during the conversation, the interpreter realizes that Maria is suffering from language deprivation. To an outside viewer, Maria’s signing is fluent and mesmerizing. However, fluent knowledge of ASL lets the interpreter realize that Maria’s signing style obscures the fact that she does not understand what is being said most of the time. Maria’s communication is very basic, and she tries to cover up for her lack of understanding by smiling and being agreeable.
Once you have time to meet with Maria, who missed her scheduled appointment slot, you go and get Maria and the interpreter. You’re still a little annoyed about the transportation problems, but that’s nothing compared to the fact that you are very nervous about this meeting. You are not sure you have ever met a person who uses ASL to communicate, and that’s anxiety provoking.
The three of you walk down the hallway silently because you are unsure how to proceed. After what feels like a very long walk, you all arrive at your office. Everyone sits down, and you turn to the interpreter to ask why Maria is here. The interpreter informs you that you should speak directly to Maria and not the interpreter. You cannot help but get flustered—there is a lot to remember! You take a deep breath, apologize to the interpreter and Maria, and begin the session.
You start by asking Maria the questions on the standard intake form, but her answers could be clearer, and despite asking her in different ways to provide the information, you need help getting your point across. You quickly remember that Maria became deaf when she was very young, and it seems she has significant language and communication gaps. Maria talks a little about her relationship with Kevin and states that while she is scared of him, she does not want anyone to know about what happened since she doesn’t want people to talk about her in the tightly-knit Deaf community.
After a while, Maria goes to the bathroom, and the interpreter suggests to you that Maria may benefit from a certified deaf interpreter (CDI). These are Deaf interpreters for the d/Deaf, who can interpret from ASL using “gesture, mime, props, drawings and other tools to enhance communication” (RID, 2022). The interpreter explains that CDIs are vital in ensuring full access to communication for d/Deaf people who have language deprivation, yet you, like most people, know nothing about CDIs. Armed with this new information, you check with your supervisor, who mentions that your agency does not have a contract with any CDIs, noting that they can only hire from a previously approved list of interpreters and says you will need to make do with the one interpreter you have.
Discussion Questions:
- The ADA requires accessibility for individuals with disabilities. There are five types of barriers to access. Attitudinal: including assumptions or bias; Organizational: including policies or practices that discriminate; Physical: including architectural design like narrow doorways, low lighting, small bathrooms; Communication: including improperly formatted documents, inaccessible language, poor design, lack of captioning; and Technology: including inaccessible websites, documents without alternative text.
- What barriers to access are you able to identify in Maria’s story?
- Thinking specifically about attitudinal barriers, what assumptions were made about Maria in this scenario? Consider applications at the macro, mezzo, and micro levels of practice.
- Collaboration between victim service providers and PWD can be a key component in ensuring safety and access for survivors with disabilities. Who might you want to collaborate with to help address some of the safety and access barriers experienced by Maria?
- Universal design means designing systems, services, and environments so that they are accessible to everyone. How do you think Universal Design could be applied within this agency?
- Empowerment theory is often applied when working with survivors of IPV and aligns well with social workers’ responsibility to promote self-determination. How do you think that you could promote self-determination and help empower Maria?
- What local and state policies might impede your ability to maintain the client’s self-determination and cause an ethical dilemma?
- Who might be members of Maria’s circle of support? How do those members support her? How might Maria’s intersectional identity impact her experience?
- How do you think Maria’s experience may have been different if you were familiar with the Deaf Community and d/Deaf people in general? What about if you were a Deaf social worker yourself?
- What power dynamics and imbalances might occur among you, Maria, and the employment and housing institutions surrounding her? How would you address them?
- Do you, as the social worker, follow the NASW ethical standard of cultural competence when providing for d/Deaf clients? What about the agency?
To Learn More:
- Sexual Violence and Intimate Partner Violence Among People with Disabilities, an overview by the Centers for Disease Control and Prevention. https://www.cdc.gov/violenceprevention/sexualviolence/svandipv.htm
- Abused and Betrayed, an NPR series about violence against people with intellectual disabilities. https://www.npr.org/2018/01/08/570224090/the-sexual-assault-epidemic-no-one-talks-about
- Many Deaf Women Aren’t Safer at Home, an article addressing the intersection of Covid stay-at-home orders and the experience of Deaf survivors. https://www.bitchmedia.org/article/deaf-women-domestic-violence-pandemic
- DeafHope – Deaf Survivor’s Story: Enduring Domestic Violence, a filmed interview with a survivor of domestic violence sharing their experience. This video is presented in ASL with closed captioning. https://www.youtube.com/watch?v=W8sNlbO4JI4&t=124s
Direct Services and Crisis Intervention
- Abused Deaf Women’s Advocacy Services (ADWAS) is the first agency in the United States to focus on empowering d/Deaf survivors of interpersonal violence. ADWAS is a model deaf-by-deaf program and also keeps a list of partnering agencies where d/Deaf survivors can find support nationally https://www.adwas.org/information/links/
- The Deaf Hotline provides 24/7 crisis intervention and support for d/Deaf individuals who have experienced domestic or sexual violence: https://thedeafhotline.org/
- RAINN, The National Sexual Assault Hotline, provides 24/7 support by chat or phone to survivors of sexual violence: https://www.rainn.org/
Tools and Toolkits
- Disability Justice Audit Tool, this interactive online tool provides an overview of disability justice and helps individuals consider its application in their agencies and practice. https://www.northwesthealth.org/djaudittool
- Partnering to Promote Safety, Access, and Inclusion for Every Survivor is a toolkit developed by the Center for Research on Ending Violence at Rutgers School of Social Work, which aims to foster ongoing collaborative relationships to promote inclusive and equitable services for all survivors. Collaboration Toolkit 2021
- Power and Control Wheel People with Disabilities and their Caregivers, this tool adapted by the National Center on Domestic and Sexual Violence highlights common power and control tactics a person might use to abuse their family member or someone in their care. https://www.communitysolutionsva.org/files/DisabledCaregiverPCwheel.pdf
- Power and Control Wheel adapted for the d/Deaf community, this tool adapted by ADWAS highlights specific power and control tactics that may be experienced by d/Deaf survivors. https://www.adwas.org/wp-content/uploads/2013/04/unhealhywheelsignatue.jpg
- Serving Deaf Survivors of Domestic and Sexual Violence, this guide produced by the Vera Institute of Justice seeks to increase individual/agency capacity for working with d/Deaf survivors. https://www.vera.org/downloads/publications/serving-deaf-survivors-domestic-sexual-violence.pdf
- Working with a Deaf Survivor: A Resource Guide, this resource guide produced by Deaf Vermonters Against Violence offers best-practice tips for working with d/Deaf survivors. http://www.deafta.org/blog/resourceguideforhearingprograms
Training and Technical Assistance
The Vera Institute for Justice manages several initiatives at the intersection of violence and disability and other underserved communities. The following may be of interest:
- End Abuse of People with Disabilities focuses specifically on building movements and cultivating leaders. Supporting organizations, leveraging resources, and advocating for change to end violence against PWD. https://www.endabusepwd.org/about-the-movement/our-work/
- National Resource Center for Reaching Victims The Resource Center is a one-stop-shop to get information and expert guidance to enhance the capacity to identify, reach, and serve all victims, especially those from communities that too often have less access to healing services and avenues to justice. https://www.reachingvictims.org/
- Deaf Action The Deaf Action Initiative is an OVW-funded training and technical assistance project designed to increase the capacity of Deaf organizations to address domestic violence, dating violence, sexual assault, and/or stalking in Deaf communities in the United States. http://www.deafta.org/about
References
ADWAS: Abused Deaf Women’s Advocacy Services. Herstory (n.d.). https://www.adwas.org/herstory/
Altman, B. M. (2011). Disability, definitions, models, classification schemes, and applications. In G. Albrecht, K. Seelman, M. Bury (Eds.), Handbook of disability studies (pp. 97–122). Thousand Oaks, CA: SAGE.
American Rescue Plan Act of 2021. 15 U.S.C. § 9001 (2021). https://www.congress.gov/117/plaws/publ2/PLAW-117publ2.pdf
Americans With Disabilities Act of 1990, Pub. L. No. 101-336, § 36.105, 104 Stat. 328 (1990).
Anti-Defamation League. (2018). A Brief History of the Disability Rights Movement. Retrieved from:https://www.adl.org/education/resources/backgrounders/disability-rights-movement
Anderson, M., Wolf Craig, K., Hall, W., & Ziedonis, D. (2016a). A pilot study of deaf trauma survivors’ experiences: Early traumas unique to being deaf in a hearing world. Journal of Child & Adolescent Trauma, 9(4), 353-358. doi:10.1007/s40653-016-0111-2
Anderson, M. L., Glickman, N. S., Mistler, L. A., & Gonzalez, M. (2016b). Working therapeutically with deaf people recovering from trauma and addiction. Psychiatric Rehabilitation Journal, 39(1), 27-32. doi:10.1037/prj0000146
Anderson, M., Sortwell, A., Craig, K. W., & Ziedonis, D. (2016c). Symptom patterns of posttraumatic stress disorder among deaf trauma survivors. JADARA, 50(1), 11-21. Retrieved from https://repository.wcsu.edu/jadara/vol50/iss1/3
Anderson, M. L., Wolf Craig, K. S., & Ziedonis, D. M. (2017a). Barriers and facilitators to deaf trauma survivors’ help-seeking behavior: Lessons for behavioral clinical trials research. The Journal of Deaf Studies and Deaf Education, 22(1), 118-130. doi:10.1093/deafed/enw066
Anderson, M. L., Wolf Craig, K. S., & Ziedonis, D. M. (2017b). Deaf people’s help-seeking following trauma: Experiences with and recommendations for the Massachusetts behavioral health care system. Psychological Trauma: Theory, Research, Practice, and Policy, 9(2), 239-248. doi:10.1037/tra0000219
Anurudran, A., Yared, L., Comrie, C., Harrison, K., & Burke, T. (2020). Domestic violence amid COVID‐19. International Journal of Gynecology & Obstetrics, 150(2), 255-256.
Araten-Bergman, T., & Bigby, C. (2020). Violence Prevention Strategies for People with Intellectual Disabilities: A Scoping Review. Australian Social Work, 76(1), 72–87. https://doi.org/10.1080/0312407x.2020.1777315
Basile, K. (2016). Stop SV: a technical package to prevent sexual violence. Division of Violence Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Basile, K. C., Breiding, M. J., & Smith, S. G. (2016). Disability and risk of recent sexual violence in the United States. American Journal of Public Health, 106(5), 928-933.
Bauman, H., Murray, J. J., & Solomon, A. (2014). Deaf gain: Raising the stakes for human diversity. Minneapolis, MN: University of Minnesota Press.
Bergen, R. (2006). Marital Rape: New Research and Directions. Harrisburg, PA: VAWnet, a project of the National Resource Center on Domestic Violence/Pennsylvania Coalition Against Domestic Violence. Retrieved from http://www.vawnet.org.
Berger, R. J. (2013) Introducing Disability Studies. Boulder, CO: Lynne Rienner Publishers, Inc.
Boness, C. L. (2016). Treatment of Deaf Clients: Ethical Considerations for Professionals in Psychology. Ethics & Behavior, 26(7), 562–585. https://doi.org/10.1080/10508422.2015.1084929
Breiding, M. J., & Armour, B. S. (2015). The association between disability and intimate partner violence in the United States, Annals of Epidemiology, 25(6), 455-457.
Buchbinder, E. (2021, July 21). VOCA Fix Passes Unanimously in the Senate, Secures Billions in Victim Service Funding. End Domestic Abuse Wisconsin. https://www.endabusewi.org/voca-fix-passes-unanimously-in-the-senate-secures-billions-in-victim-service-funding/
Burke, T. (2017, November 10). #MeToo was started for black and brown women and girls. They’re still being ignored. Washington Post. https://www.washingtonpost.com/news/post-nation/wp/2017/11/09/the-waitress-who-works-in-the-diner-needs-to-know-that-the-issue-of-sexual-harassment-is-about-her-too/
Carlson, B., Worden, A., van Ryn, M., and Bachman, R.(2003). Violence Against Women: Synthesis of Research for Practitioners (Document No.: 199577). U.S. Department of Justice. https://www.ojp.gov/pdffiles1/nij/grants/199577.pdf
Centers for Disease Control and Prevention (CDC), (n.d.). Disability impacts all of us. https://www.cdc.gov/ncbddd/disabilityandhealth/infographic-disability-impacts-all.html#:~:text=61%20million%20adults%20in%20the,is%20highest%20in%20the%20South.
Centers for Disease Control and Prevention. (2022, February 9). Rape prevention and education (RPE) program. Centers for Disease Control and Prevention. https://www.cdc.gov/violenceprevention/sexualviolence/rpe/index.html
Centers for Disease Control and Prevention (CDC), (n.d.). Sexual violence and intimate partner violence among people with disabilities. https://www.cdc.gov/violenceprevention/sexualviolence/svandipv.html
Centers for Disease Control and Prevention (2008). Racial/Ethnic disparities in self-rated health status among adults with and without disabilities—United States, 2004-2006. Morbidity and Mortality Weekly Report Weekly, 57(39), 1069-1073
Certified deaf interpreter. Registry of Interpreters for the Deaf. (2021, August 31). Retrieved from https://rid.org/rid-certification-overview/available-certification/cdi-certification/
Collins, J. & Murphy, G. H. (2021). Detection and prevention of abuse of adults with intellectual and other developmental disabilities in care services: A systemic review. Journal of Applied Research in Intellectual Disabilities, 35(2), 338-373.
Congress Profiles | US House of Representatives: History, Art & Archives. (n.d.). https://history.house.gov/Congressional-Overview/Profiles/98th/
Cramer, E. P., Gilson, S.F., & DePoy, E. (2003). Women with disabilities and experiences of abuse. Journal of Human Behavior in the Social Environment, 7, 183-199.
Crenshaw, K. (1991). Mapping the margins: intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241-1300.
Curry, M. A., Powers, L. E., & Oschwald, M. (2004). Development of an abuse screening tool for women with disabilities. Journal of Aggression, Maltreatment & Trauma, 8(4), 123–141. https://doi.org/10.1300/J146v08n04_06
The Deaf Hotline. The Deaf Hotline. (n.d.). https://thedeafhotline.org/
Department of Justice, Office of Justice Programs. (2020) National Crime Victimization Survey, 2015-2019. Bureau of Justice Statistics. https://bjs.ojp.gov/content/pub/pdf/cv19.pdf
Department of Justice, National Institute of Justice. (2016, May). Five Things About Violence Against American Indian and Alaska Native Women and Men. https://www.ojp.gov/pdffiles1/nij/249815.pdf
Department of Justice. (n.d.). Office on Violence Against Women. https://www.justice.gov/ovw/about-office
Department of Justice, Office of Public Affairs. (2017, January 13) Justice Department Awards $500,000 to Initiate Video-Based Services for Deaf Victims. [Press release] https://www.justice.gov/opa/pr/justice-department-awards-500000-initiate-video-based-services-deaf-victims
Department of Justice, Office of Justice Programs. (n.d.). Funding & awards: OVC. Office for Victims of Crime. https://ovc.ojp.gov/funding
Department of Justice, Office of Justice Programs, Office of Victims of Crime. (2022, April 4). OVC FY 2022 Advancing the Use of Technology to Assist Victims of Crime. Washington, DC. https://ovc.ojp.gov/funding/fy-2022/O-OVC-2022-171237.pdf
Dubin, M. (2007). Domestic violence shelters and the ADA. http://www.ncdsv.org/images/DVsheltersADA.pdf
Dunn, L. (n.d.). Vilissa Thompson, Creator of #DisabilityTooWhite, Brings An Intersectional Lens to Disability Advocacy. https://www.inclusionhub.com/articles/vilissathompson
Evans, S. M. (2015). Women’s liberation: Seeing the revolution clearly. Feminist Studies, 41(1), 138-149.
Equal Employment Opportunity Commission (1997). Fact Sheet: Disability Discrimination. https://www.eeoc.gov/laws/guidance/fact-sheet-disability-discrimination
Family Violence Prevention and Services Act. 42 U.S.C.§ 10401 (2010). https://www.govinfo.gov/content/pkg/PLAW-111publ320/pdf/PLAW-111publ320.pdf
Family Violence Prevention and Services Improvement Act of 2021, H.R. 2119, 117 Cong. (2021). https://www.congress.gov/117/bills/hr2119/BILLS-117hr2119pcs.pdf
Fernandes-Alcantara, A. L., & Billings, K. C. (2021). Family Violence Prevention and Services Act (FVPSA): Background and Funding.
Findley, P. A., Plummer, S.-B., & McMahon, S. (2016). Exploring the experiences of abuse of college students with disabilities. Journal of Interpersonal Violence, 31(17), 2801–2823. https://doi-org.proxy.libraries.rutgers.edu/10.1177/0886260515581906.
Freeman, A. (2003). Eye movement and desensitization reprocessing: An effective technique for post-traumatic disorders in hearing impaired persons. JADARA: a Journal for Professionals Networking for Excellence in Service Delivery with Individuals who are Deaf or Hard of Hearing, 37(1), 32-42.
Friedmann, N., & Rusou, D. (2015). Critical period for first language: the crucial role of language input during the first year of life. Current opinion in neurobiology, 35, 27–34. https://doi.org/10.1016/j.conb.2015.06.003
Garberoglio, C. L., Cawthon, S., & Sales, A. (2017). Deaf People and Educational Attainment in the United States: 2017. Washington, DC: U.S. Department of Education, Office of Special Education Programs, National Deaf Center on Postsecondary Outcomes.
Ghafoori, B., Barragan, B., & Palinkas, L. (2014). Mental health service use among trauma-exposed adults: A mixed-methods study. The Journal of Nervous and Mental Disease, 202(3), 239-246. doi:10.1097/NMD.0000000000000108
Gilson, S.F., DePoy, E., & Cramer, E. P. (2001). Linking the assessment of self-reported functional capacity with abuse experiences of women with disabilities. Violence Against Women, 7, 418-431.
Glickman, N. S., & Gulati, S. (2003). Mental health care of deaf people: A culturally affirmative approach. Lawrence Erlbaum Associates.
Gover, & Moore, A. M. (2021). The 1994 Violence Against Women Act: A historic response to gender violence. Violence Against Women, 27(1), 8–29. https://doi.org/10.1177/1077801220949705
Hall, M. L., Eigsti, I. M., Bortfeld, H., & Lillo-Martin, D. (2017). Auditory deprivation does not impair executive function, but language deprivation might: Evidence from a parent-report measure in Deaf native signing children. Journal of Deaf Studies and Deaf Education, 22(1), 9–21. https://doi.org/10.1093/Deafed/enw054
Hall, M. L., Hall, W. C., & Caselli, N. K. (2019). Deaf children need language, not (just) speech. First Language, 39(4), 367-395. 10.1177/014272371983410
Hall, W. C., Smith, S. R., Sutter, E. J., Dewindt, L. A., & Dye, T. D. V (2018). Considering parental hearing status as a social determinant of Deaf population health: Insights from experiences of the “dinner table syndrome”. PloS One, 13(9), e0202169. https://doi.org/10.1371/journal.pone.0202169
Hall, W. C. (2017). What you don’t Know can hurt you: The risk of language deprivation by impairing sign language development in Deaf children. Maternal and Child Health Journal, 21(5), 961-965. https://doi.org/10.1007/s10995-017-2287-y
Hall, W. C., Levin, L. L., & Anderson, M. L. (2017b). Language deprivation syndrome: a possible neurodevelopmental disorder with sociocultural origins. Social Psychiatry and Psychiatric Epidemiology, 52(6), 761-776. https://doi.org/10.1007/s00127-017-1351-7
Hahn, J.W., McCormick, M.C., Silverman, J.G., Robinson, E.B., & Koenen, K.C. (2014). Examining the impact of disability status on intimate partner violence victimization in a population sample. Journal of Interpersonal Violence, 29(17), 3063-3085.
Haydon, A, A., McRee, A.L., & Halpern, C.T. (2011). Unwanted sex among young adults in the United States: The role of physical disability and cognitive performance. Journal of Interpersonal Violence, 26, 3476-3493.
Hassouneh-Phillips, D. & Curry, M.A. (2002). Abuse of women with disabilities: State of the science. Rehabilitation Counseling Bulletin, 45(2), 96-104.
Hearing Loss Association of America (HLAA). 2018. Hearing Loss: Facts and Statistics https://www.hearingloss.org/wpcontent/uploads/HLAA_HearingLoss_Facts_Statistics.pdf?pdf=FactStats
History of Women in the U.S. Congress. (n.d.). https://cawp.rutgers.edu/facts/levels-office/congress/history-women-us-congress
Hollomotz, A. (2013). Disability, oppression, and violence: Towards a sociological explanation. Sociology, 47(3), 477-493.
Hughes, K., Bellis, M. A., Jones, L., Wood, S., Bates, G., Eckley, L., McCoy, E., Mikton, C., Shakespeare, T., & Officer, A. (2012). Prevalence and risk of violence against adults with disabilities: a systematic review and meta-analysis of observational studies. The Lancet, 379(9826), 1621-1629
Humphries, T., Kushalnagar, P., Mathur, G., Napoli, D. J., Padden, C., Rathmann, C., & Smith, R. (2012). Language acquisition for deaf children: Reducing the harms of zero tolerance to the use of alternative approaches. Harm Reduction Journal, 9, 16. https://doi.org/10.1186/1477-7517-9-16
Johnson, P., Cawthon, S., Fink, B., Wendel, E., Schoffstall, S., & Johnson, P. (2018). Trauma and resilience among Deaf individuals. Journal of Deaf Studies and Deaf Education, 23(4), 317-330.https://doi.org/10.1093/Deafed/eny024
Kamp, J., (2020). Patriarchy and Gender Law in Ancient Rome and Colonial America. Iowa Historical Review 8(1), 43-57. doi: https://doi.org/10.17077/2373-1842.1072
Kattari, S. K., Olzman, M., & Hanna, M. D. (2018). “You look fine!” Affilia, 33(4), 477–492. https://doi.org/10.1177/0886109918778073
Laney, G. P. (2010). Violence against women act: History and federal funding. In Stickle, D. V. (Ed.), Women’s Issues: Economic, Societal, and Personal (pp1-48). Nova Publishers.
Mailhot Amborski, A., Bussières, E.-L., Vaillancourt-Morel, M.-P., & Joyal, C. C. (2021). Sexual Violence Against Persons With Disabilities: A Meta-Analysis. Trauma, Violence, & Abuse. https://doi.org/10.1177/1524838021995975
Mansell, S., Sobsey, D., & Calder, P. (1992). Sexual abuse treatment for persons with developmental disabilities. Professional Psychology: Research and Practice, 23(5), 404–409.
Marques, E. S., Moraes, C. L. D., Hasselmann, M. H., Deslandes, S. F., & Reichenheim, M. E. (2020). Violence against women, children, and adolescents during the COVID-19 pandemic: overview, contributing factors, and mitigating measures. Cadernos de Saude Publica, 36, e00074420.
Mazza, M., Marano, G., Lai, C., Janiri, L., & Sani, G. (2020). Danger in danger: Interpersonal violence during COVID-19 quarantine. Psychiatry Research, 289, 113046.
McFarlane, J., Hughes, R. B., Nosek, M. A., Groff, J. Y., Swedlend, N., & Dolen Mullen, P. (2001). Abuse Assessment Screen – Disability (AAS-D): Measuring frequency, type, and perpetrator of abuse toward women with physical disabilities. Journal of Women’s Health & Gender-Based Medicine, 10 (9), 861-866.
McNamara, B. (2018, May 25). This hashtag makes sure disabled people are heard in the #MeToo movement. Teen Vogue. https://www.teenvogue.com/story/hashtag-makes-sure-disabled-people-are-heard-in-the-me-too-movement
Meek, D. R. (2020). Dinner Table Syndrome: A phenomenological study of Deaf individuals’ experiences with inaccessible communication. Qualitative Report, 25(6), 1676-1694.
Mikton, C., Maguire, H., & Shakespeare, T. (2014). A systematic review of the effectiveness of interventions to prevent and respond to violence against persons with disabilities. Journal of Interpersonal Violence, 29(17), 3207–3226. https://doi.org/10.1177/0886260514534530
Mitra, M., & Mouradian, V. E. (2014). Intimate partner violence in the relationships of men with disabilities in the United States: relative prevalence and health correlates. Journal of Interpersonal Violence, 29(17), 3150–3166. https://doi.org/10.1177/0886260514534526
Mullen, C. (2018). Places of public accommodation: Americans with Disabilities and the battle for Internet accessibility. Drexel L. Rev., 11, 745.
National Association of the Deaf. (2019). Community and culture – frequently asked questions. https://www.nad.org/resources/american-sign-language/ communityandculture-frequently-asked-questions/
National Association of Social Workers (2015). Standards and indicators for cultural competence in social work practice. NASW.
National Child Traumatic Stress Network, Adapted Trauma Treatment Standards Work Group & Subgroup on the Deaf and Hard of Hearing. (2004). Facts on trauma and Deaf children. https://www.nctsn.org/resources/facts-trauma-and-deaf-children
National Democratic Institute (2022, March 28). From “nothing about us without us” to “nothing without us.”https://www.ndi.org/our-stories/nothing-about-us-without-us-nothing-without-us
National Institute on Deafness and Other Communication Disorders. (2010). NIDCD Fact Sheet: Tinnitus. https://permanent.fdlp.gov/gpo49797/TinnitusFS.pdf
National Network to End Domestic Violence. (2022, March). Violence Against Women Act (VAWA) and Related Programs Appropriations for Fiscal Years 19, 20, 21, and 22. Washington, DC. https://nnedv.org/wp-content/uploads/2022/03/FY22-Appropriations-Chart-Final-FY22-Budget-.pdf
The New York Times (1983, October 22). Opinion | Letter on Domestic Violence; Troubled Families Need Help, Not Studies. The New York Times. https://www.nytimes.com/1983/10/22/opinion/l-letter-on-domestic-violence-troubled-families-need-help-not-studies-248296.html
Niolon, P. H., Kearns, M., Dills, J., Rambo, K., Irving, S., Armstead, T. L., & Gilbert, L. (2017). Preventing intimate partner violence across the lifespan : a technical package of programs, policies, and practices. Division of Violence Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Obinna, J., Krueger, S., Osterbaan, C., Sadusky, J. M., & DeVore, W. (2006, February). Understanding the needs of the victims of sexual assault in the deaf … https://www.ojp.gov/pdffiles1/nij/grants/212867.pdf
Office on Violence Against Women. (2021, May 7). OVW FY 2022 Congressional Justification. The United States Department of Justice. https://www.justice.gov/jmd/page/file/1398501/download
Office on Violence Against Women. (2022, March). Office on Violence Against Women FY 2023 President’s Budget Request. Washington, DC. https://www.ojp.gov/sites/g/files/xyckuh241/files/media/document/fy23ovwpresbudgetoverview.pdf
Onwuachi-Willig, A. (2018-2019). What about #UsToo?: The invisibility of race in the #MeToo movement. Yale Law Journal Forum, 128, 105-120.
Plummer, S. & Findley, P. (2012). Women with disabilities’ experience with physical and sexual abuse: A review of the literature and implications for the field. Trauma, Violence, & Abuse 13(1), 15-29.
Porter, J. L., & Williams, L. M. (2011). Auditory status and experiences of abuse among college students. Violence and Victims, 26(6), 788-798. doi:10.1891/0886-6708.26.6.788
Price, J. (2011). The Seeds of a Movement— Disabled Women and Their Struggle to Organize. In S. Batliwala (Ed.), Changing their world: Concepts and practices of women’s movements (2nd edition). essay, Association for Women’s Rights in Development (AWID).
Sacco, L. & Hanson, E. (2019) The Violence Against Women Act (VAWA): Historical Overview, Funding, and Reauthorization. Congressional Research Service.
Sacco, L. (2021). The crime victims fund : federal support for victims of crime. Congressional Research Service.
Sapire, Ostrowski, J., Maier, M., Samari, G., Bencomo, C., & McGovern, T. (2022). COVID-19 and gender-based violence service provision in the United States. PloS One, 17(2), e0263970–e0263970. https://doi.org/10.1371/journal.pone.0263970
Schalk, S. D. (2022). Black disability politics. Duke University Press. https://doi.org/10.1515/9781478027003
Schenkel, L. S., Rothman-Marshall, G., Schlehofer, D. A., Towne, T. L., Burnash, D. L., & Priddy, B. M. (2014). Child maltreatment and trauma exposure among deaf and hard of hearing young adults. Child Abuse and Neglect, 38(10), 1581-1589. doi:10.1016/j.chiabu.2014.04.010
Schild, S., & Dalenberg, C. J. (2011). Trauma exposure and traumatic symptoms in deaf adults. Psychological Trauma: Theory, Research, Practice, and Policy, 4(1), 117-127. doi:10.1037/a0021578
Slayter, E. M., Kattari, S. K., Yakas, L., Singh, R. C. B., Goulden, A., Taylor, S., Wernick, L. J., Simmons, L. D., & Prince, D. (2022). Beyond Ramps, Curb Cuts, and Captions: A Call for Disability Justice in Social Work. Social Work (New York), 68(1), 89–92. https://doi.org/10.1093/sw/swac045
Smith, D.L. (2007). Disability, gender, and intimate partner violence: Relationships from the Behavioral Risk Factor Surveillance System. Sexuality and Disability 26, 15-28.
Stutts L.A. (2022) Sexual Abuse Among Individuals with Disabilities. In: Geffner R., White J.W., Hamberger L.K., Rosenbaum A., Vaughan-Eden V., Vieth V.I. (eds) Handbook of Interpersonal Violence and Abuse Across the Lifespan. Springer, Cham.
Swedlund, N.P. & Nosek, M.A. (2000). An exploratory study on the work of independent living centers to address abuse of women with disabilities. Journal of Rehabilitation, 66, 57-64.
Thompson, V., Ellmann, N., Cokely, R., & Allsbrook, J. F. (2021, February 12). Sexual violence and the disability community. Center for American Progress. https://www.americanprogress.org/article/sexual-violence-disability-community/
Tyiska, C. (1998). Working with victims of crime with disabilities. U.S. Dept. of Justice, Office of Justice Programs, Office for Victims of Crime. https://www.ncjrs.gov/ovc_archives/factsheets/disable.htm
Tomsa, R., Gutu, S., Cojocaru, D., Gutierrez-Bermejo, B. Flores, N., & Jenaro, C. (2021). Prevalence of sexual abuse in adults with intellectual disabilities: Systemic review and meta-analysis. International Journal of Environmental Research and Public Health, 18, 1980.
United Nations, Office of the High Commissioner for Human Rights(1993). Declaration on the Elimination of Violence against Women. Office of the High Commissioner for Human Rights. https://www.ohchr.org/en/instruments-mechanisms/instruments/declaration-elimination-violence-against-women
United States Senate, Committee on Appropriations. (2022, March 9). Summary Commerce, Justice, Science, and Related Agencies Fiscal Year Appropriations Bill [Press release]. https://www.appropriations.senate.gov/imo/media/doc/CJS2.pdf
van der Kolk, B. (2015). The body keeps the score: brain, mind, and body in the healing of trauma. Penguin Books.
Van Eck, C.A. (2017). Changing the Message: Battered Women’s Advocates and Their Fight Against Domestic Violence at the Local, State, and Federal Level, 1970-1990s. ProQuest Dissertations Publishing.
Vera Institute of Justice [DeafHope Team]. (2022, April 7). Deaf Action Townhall November 2021 [Video]. YouTube. https://www.youtube.com/watch?v=qoscvxvu3b8
Violence Against Women Act Reauthorization Act of 2022. 34 U.S.C. § 12291 (2022). https://www.congress.gov/bill/117th-congress/house-bill/2471/text
Violence Against Women Reauthorization Act of 2013. 42 U.S.C. § 13701 (2013). https://www.congress.gov/113/plaws/publ4/PLAW-113publ4.pdf
VOCA Fix to Sustain the Crime Victims Fund Act of 2021. 34 U.S.C. § 10101 (2021). https://www.congress.gov/117/plaws/publ27/PLAW-117publ27.pdf
Weldon. (2002). Protest, policy, and the problem of violence against women : a cross-national comparison. University of Pittsburgh Press.
The White House. Executive Order On Advancing Racial Equity and Support for Underserved Communities Through the Federal Government. (2021, January 21). https://www.whitehouse.gov/briefing-room/presidential-actions/2021/01/20/executive-order-advancing-racial-equity-and-support-for-underserved-communities-through-the-federal-government/
The White House (2021, May 18). Memorandum on Restoring the Department of Justice’s Access-to-Justice Function and Reinvigorating the White House Legal Aid Interagency Roundtable. https://www.whitehouse.gov/briefing-room/presidential-actions/2021/05/18/memorandum-on-restoring-the-department-of-justices-access-to-justice-function-and-reinvigorating-the-white-house-legal-aid-interagency-roundtable/
The White House. (2022, March 16). Fact Sheet: Reauthorization of the Violence Against Women Act (VAWA) [Press release]. https://www.whitehouse.gov/briefing-room/statements-releases/2022/03/16/fact-sheet-reauthorization-of-the-violence-against-women-act-vawa/
Wanjiru, Q. (2021). Causes and effects of gender-based violence: A critical literature review. Journal of Gender related Studies, 2(1), 43-53.
Wiseman, P., & Watson, N. (2021). “Because I’ve got a learning disability, they don’t take me seriously:” Violence, wellbeing, and devaluing people with learning disabilities. Journal of Interpersonal Violence, 37(13-14). 0886260521990828.
- Interpersonal Violence (IPV)', which may include physical assault, sexual assault, stalking, and domestic violence. ↵
- The authors will primarily use PWD in order to identify people with disabilities. Our language throughout will change from person-first language to identity-first language to recognize the changing ways we address disability. ↵
- In the Deaf community, lowercase d indicates someone who has hearing loss, but may not culturally identify as Deaf. Capitalized D Deaf indicates someone who knows and uses ASL and identifies as culturally Deaf. This chapter will use both terms. ↵
- Positionality refers to the social, cultural, political, and personal contexts that make up each individual’s life experiences, power, and viewpoints. ↵
- According to “section 40002(a) of the Violence Against Women Act of 1994 (42 U.S.C. 13925(a)). The term “underserved populations” means populations who face barriers in accessing and using victim services, and includes populations underserved because of geographic location, religion, sexual orientation, gender identity, underserved racial and ethnic populations, populations underserved because of special needs (such as language barriers, disabilities, alienage status, or age), and any other population determined to be underserved by the Attorney General or by the Secretary of Health and Human Services, as appropriate. ↵
- American Indian and Alaska Natives experience high rates of interpersonal violence across their lifetime, often perpetrated by non-native harm-doers and also experience disability at high rates (DOJ, 2016; CDC, 2008). ↵
- People with hearing loss who know ASL and adhere to the values and norms of the Deaf community identify themselves as “big D Deaf” or culturally Deaf (National Association of the Deaf, 2019). Another common term is ‘Hard of Hearing’ (HH), which denotes someone who has mild to moderate hearing loss. People who identify as HH may or may not use amplification technology like hearing aids and cochlear implants that allow them to hear to some degree. Like d/Deaf people, HH people know and use ASL, adhere to Deaf culture, and identify as a member of the d/Deaf community (National Association of the Deaf, 2019). This chapter uses d/Deaf to denote people with hearing loss, as anyone with a hearing loss can join the Deaf community at any time, as well as promote solidarity among people with hearing loss. ↵
- Deaf Gain redefines hearing differences as positive; Deaf Gain highlights the ways in which humanity has benefited from the existence of deaf people and sign language throughout recorded human history. ↵
- Prelingual deafness means being born with hearing loss or becoming deaf before learning spoken language. ↵
- Intimate Partner Violence is abuse or aggression that occurs in a romantic relationship by a former or current partner or spouse (CDC, n.d.). Intimate Partner Violence falls under the interpersonal violence umbrella. ↵

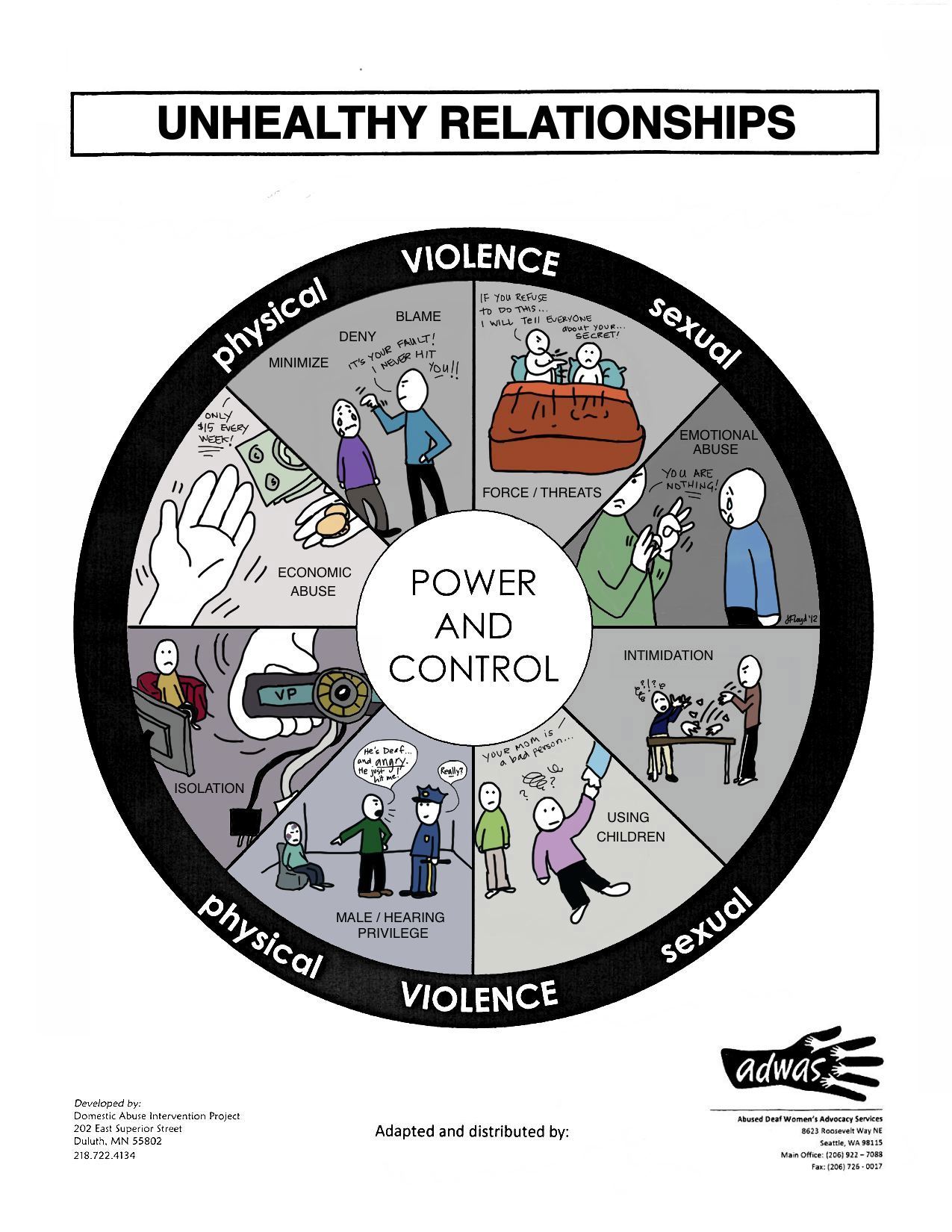{kind=link}