
A note on race and human ancestry
Humans like to categorize things, including other humans. And the concept of race permeates nearly every part of life in the United States in one way or another.
Early geneticists assumed that phenotypic variation among races arose through the dispersal of human populations and parallel divergence from a common ancestor. This assumption often formed the basis for egregious social practices designed to maintain power for one racial or ethnic group over another.
But there’s a lot of data to show that this assumption just isn’t true.
First of all, even self-identification of race is very subjective and differs from country to country across the world. For example, people who self-identify as white in Brazil often have more African ancestry than people who self-identify as Black in the United States.[1]
In addition, there is more genetic variation within racial groupings than there is between people of different races. In other words, in a genomic comparison of your DNA with someone of the same race and someone of a different race, you’re just as likely to be a closer genetic match to the person of a different race9. This is especially true for the oldest African populations, which tend to be far more genetically diverse than populations founded later in human expansion.
And finally, genomic data reveals so much admixture that there are no reproductive separations among different racial groups. Instead, people tend to be most closely related to others with proximal geographic ancestry, but there does not seem to be any discrete separation. Human variation exists along a continuous variation, mostly along the exact migration paths described back in Figure 11. The haplotypes used to predict geographic ancestry are hyperlocal: they do not fall along the borders one might expect for racial separation, and different haplotypes have overlapping geographies.
These data collectively form the scientific basis for the statement that there is no genetic separation of racial groups.
Despite this, race continues to be used as a proxy for genetics in medicine, sometimes with good intentions but often to patients’ detriment. Historically, clinical trials were overwhelmingly performed using white male patients. This led to treatments that worked well in white male patients but sometimes less well for other populations. In recent years, efforts have been made to increase diversity in clinical trials, with efforts to specifically recruit BIPOC patients as well as women and gender-diverse patients historically underrepresented in clinical trials.[2] But identifying patients solely by race does not necessarily lead to improved outcomes either, since race is not a good proxy for genetics.
With that being said, a lack of genetic basis for race does not mean that race is not real. Race and cultural influences can have a profound effect on human health: for just two examples, Black women have a three-fold higher chance of dying in childbirth compared with white women, and there is strong evidence for disparities in how pain is treated and managed in BIPOC populations compared with white populations[3] [4]
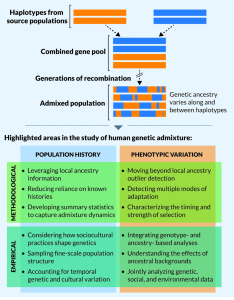
An increased understanding of both genetic and social/cultural influences on human health is necessary to improve outcomes. The bottom panel of Figure 16 offers some suggestions for the use of genetic and genomic data.
Test Your Understanding
- Templeton, A. R. Biological Races in Humans. Stud. Hist. Philos. Biol. Biomed. Sci. 44, 262–271 (2013). ↵
- Igwe, J. et al. Opportunities to Increase Science of Diversity and Inclusion in Clinical Trials: Equity and a Lack of a Control. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 12, e030042 (2023). ↵
- Njoku, A., Evans, M., Nimo-Sefah, L. & Bailey, J. Listen to the Whispers before They Become Screams: Addressing Black Maternal Morbidity and Mortality in the United States. Healthcare 11, 438 (2023). ↵
- Salmond, S. & Dorsen, C. Time to Reflect and Take Action on Health Disparities and Health Inequities. Orthop. Nurs. 41, 64–85 (2022) ↵

{kind=link}